
Abstract. “Intermittent fasting” has entered public discourse as a single category, but very different practices live under the same label — from daily 16:8 to the five-days-a-month fasting-mimicking diet. On the daily protocols the literature is by now clear: at equal calories, they don’t drive more weight loss than a classic diet, and the “extra” metabolic benefits are small or extrapolated from mice. The case that holds up clinically is the FMD: five days a month of heavily reduced intake, with replicated human data on insulin sensitivity, inflammatory markers, and cardiometabolic profile. The molecular rationale runs through mTOR — the amino-acid and insulin sensor that periodic fasting modulates over a long enough stretch, while sixteen hours of daily fasting modulates only briefly. A disproportionate enthusiasm remains: 16:8 autophagy, white-fat browning, “demonstrated” longevity are still mostly rodent stories. Here I try to separate the solid case (FMD, early time-restricted eating for specific profiles) from the noise.
When an idea actually works in medicine and nutrition, it usually doesn’t need evangelists. When it does, it’s worth looking carefully.
Intermittent fasting reached the general public around 2012-2013 with Michael Mosley’s The Fast Diet and the 5:2 protocol, and from there it never stopped: 16:8, 18:6, 20:4, OMAD, alternate-day fasting, fasting-mimicking diet, prolonged fasts of three, five, seven days. Every variant has its book, its influencer, its biological rationale told as if it were the answer.
Yet if you go back to the basic question — which intermittent fasting does something unique that a good normal diet doesn’t? — the answer that emerges from the better literature of the last ten years is one and specific: the protocol with the most convincing clinical data isn’t 16:8, but the fasting-mimicking diet developed by Valter Longo’s lab at USC. Five days a month, not sixteen hours a day. It’s a different thing, and it has to be told as such.
In this article I try to put things in order. What we mean by intermittent fasting, why the cornerstone is still the caloric deficit, where the FMD breaks away from the rest, what holds up of the molecular rationale (mTOR, insulin sensitivity, inflammation), and for whom this practice is simply wrong.
1. What “intermittent fasting” means¶
Under the umbrella of intermittent fasting live very different practices. It’s worth distinguishing them, because talking about “IF” in general means almost nothing.
Time-restricted eating (TRE). You eat in a reduced window — 8, 6, or 4 hours — and fast in the rest. The most studied variants are 16:8 and 18:6. There’s an early version (eTRE), with the window pushed to the morning and closed by mid-afternoon.
Alternate-day fasting (ADF). You alternate normal days with days at ≤500 kcal.
5:2 protocol. Five days of free eating and two days a week of strong hypocaloric intake (500-600 kcal).
OMAD (one meal a day). A single meal in 24 hours. Extreme, popular in biohacking circles, rarely studied in serious clinical trials.
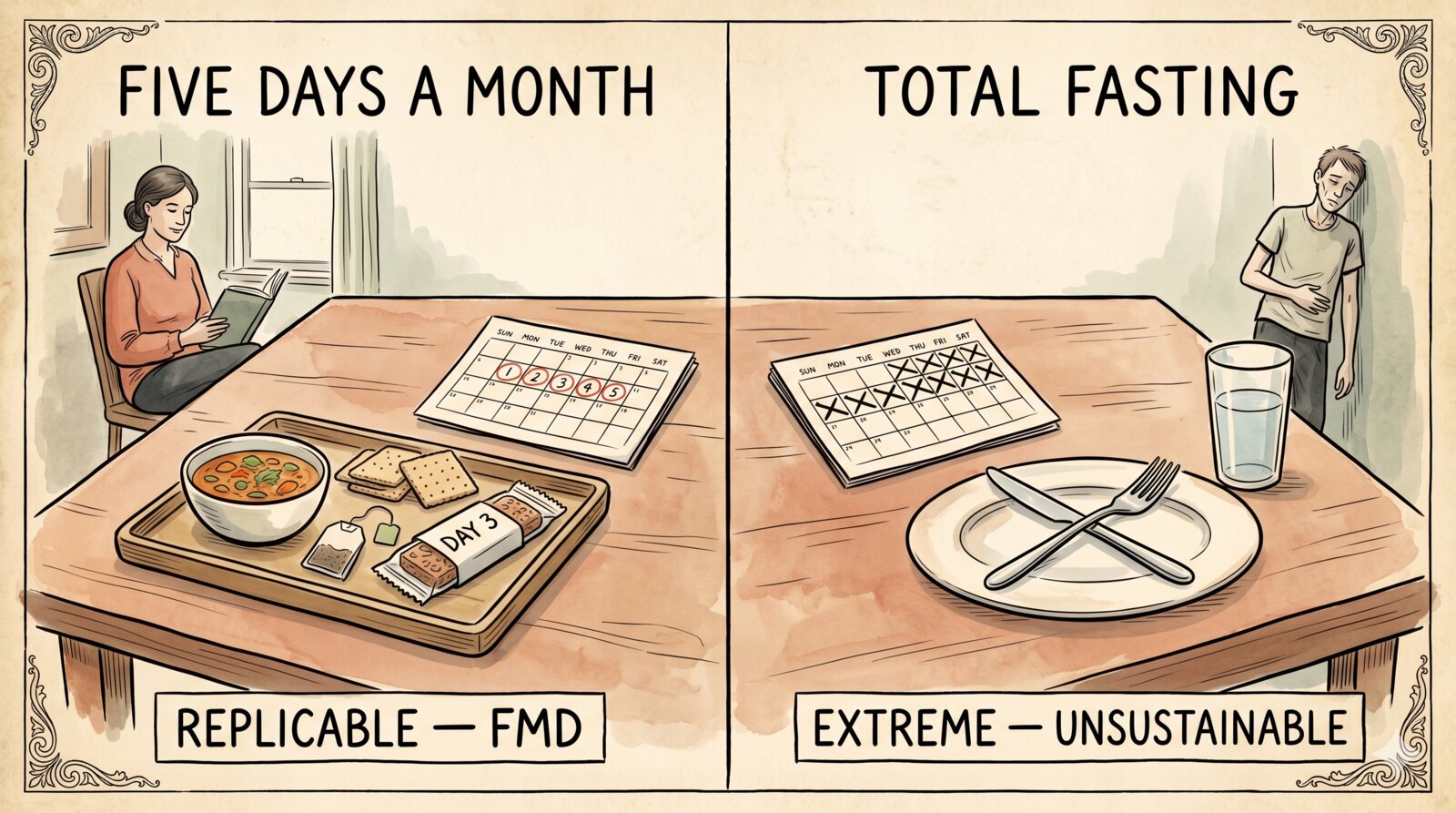
Fasting-mimicking diet (FMD). Five days a month of heavily reduced, low-protein intake (700-1100 kcal/day), then 25 days of normal eating. A specific, patented protocol, sold commercially under the name ProLon. It is the case apart of this whole article.
Prolonged fasts. Three, five, seven days or more on water or broth alone. Practiced in some centers under medical supervision; popular in the wellness world without any supervision. Sparse clinical literature, numerous contraindications.
Confusing TRE 16:8 with a five-day FMD protocol or with a prolonged fast is like confusing a walk with a marathon: same verb, different activities, different evidence.
2. The cornerstone is still the caloric deficit¶
On the daily protocols — 16:8, ADF, 5:2 — the point that randomized controlled trials by now agree on is simple: at equal calories, intermittent fasting doesn’t drive more weight loss than a normal hypocaloric diet.
Trepanowski and colleagues (JAMA Internal Medicine, 2017 — PMID 28459931) randomized 100 obese adults to alternate-day fasting, 25% caloric restriction, or control, for twelve months. Weight loss was overlapping between alternate-day fasting and continuous restriction (around 6%); adherence paradoxically worse in the fasting group.
Liu and colleagues (N Engl J Med, 2022 — PMID 35443107) randomized 139 obese adults to TRE 8:16 with 25% caloric restriction or 25% caloric restriction without time constraints, for twelve months. No significant difference in weight, no relevant difference on blood pressure, lipids, glucose.
Lowe and colleagues (TREAT, JAMA Internal Medicine, 2020 — PMID 32986097) compared TRE 16:8 with three regular meals over twelve weeks: no added benefit from TRE on body composition, and a slightly greater loss of lean mass in the fasting arm — one of the least advertised points of this practice.
When the calorie count is controlled, daily protocols don’t offer an edge on weight. When in practice they do drive weight loss, it’s because eating in an eight-hour window means eating less total than eating across the whole day. Caloric deficit, packaged differently.
It isn’t a detail. It means the active principle of these protocols is not fasting: it’s the reduction in calories. Everything else is a behavioral strategy — useful for those who find it compatible, irrelevant for those who don’t.
3. The fasting-mimicking diet: the protocol with real clinical data¶
Here the conversation changes. The FMD is not a “biohacking trend”: it’s a specific protocol, developed by Valter Longo, with randomized trials on measurable outcomes.
The protocol: five days a month of heavily reduced intake, low in protein and sugars, rich in unsaturated fats and fiber, with caloric intake between 700 and 1100 kcal per day. The other 25 days you eat normally. It’s a periodic fast, not a daily one. The difference from 16:8 is qualitative, not just quantitative: five consecutive days of strong restriction are a metabolic stress prolonged enough to activate cellular programs (drop in IGF-1, drop in mTOR activity, metabolic reprogramming) that sixteen hours of overnight fasting do not reach.
The key study is Wei and colleagues, Science Translational Medicine 2017 (PMID 28202779): randomized cross-over trial, 100 healthy adults, three FMD cycles over three months. Results in the FMD group versus control:
- Weight and waist circumference: modest but significant reduction, maintained at three months.
- Blood pressure: average reduction of 4-5 mmHg systolic in pre-hypertensive subjects.
- IGF-1: marked reduction. This is an important mechanistic data point: IGF-1 is the main downstream effector of the GH/insulin axis, chronically high levels are associated with greater oncological risk in epidemiological studies, and it’s one of the central biomarkers of aging biology.
- C-reactive protein (CRP): reduction in subjects with elevated baseline values. It’s a marker of low-grade systemic inflammation, associated with cardiovascular and metabolic risk.
- HOMA-IR and fasting glucose: improvement in subjects whose metabolism was already at the edge.
The most solid signal, in other words, concerns two dimensions that are the clinical heart of the conversation: insulin sensitivity and inflammation. They are the two variables on which periodic fasting — unlike daily 16:8 — produces an effect that breaks away from the caloric deficit alone, and it’s plausible to attribute it to the intensity and duration of the restriction (five consecutive days) rather than to the periodicity of the eating windows.
The animal rationale is consistent. Brandhorst and colleagues’ work (Cell Metabolism 2015 — PMID 26094889) — the first systematic study of FMD in mice — showed reduction of visceral fat mass, IGF-1 drop, improvement in insulin sensitivity, reduction of inflammatory markers, increased regeneration of hematopoietic and neural stem cells, and in mice an extension of mean lifespan. The animal pattern is solid. The human translation is partial and for now limited to biomarkers, but closer to the murine model than what happens with 16:8.
The caveats deserve equal precision.
First: the improvements in human trials largely disappear if the practice is interrupted. It’s a period effect, not a stable change. It has to be repeated over time to be maintained.
Second: the improved biomarkers are not clinical outcomes. Mortality, cardiovascular events, tumor incidence — the end-points that really matter in preventive medicine — have not yet been measured for FMD on a large scale and over long timeframes. Larger trials are underway, some in oncology (FMD has a plausible biological logic as a chemotherapy adjuvant, especially in IGF-1-dependent tumors), but as of today, talk of “FMD that lengthens human life” is journalism, not science.
Third: ProLon, the commercial product, is a convenience choice. The protocol logic can be replicated with normal food at much lower cost — the practical obstacle is composition (low protein, low glycemic index, high micronutrient density) and the discipline of five consecutive days. The product makes adherence less fragile, not better in principle.
That said, among all the protocols under the “intermittent fasting” label, the FMD is the one with the most solid scientific base. Not because it’s magical, but because it has been studied better and with more relevant outcomes.
4. mTOR: the cellular energy sensor¶
To understand why a periodic five-day fast produces different clinical signals than a daily sixteen-hour fast, it’s worth briefly entering mTOR biology.
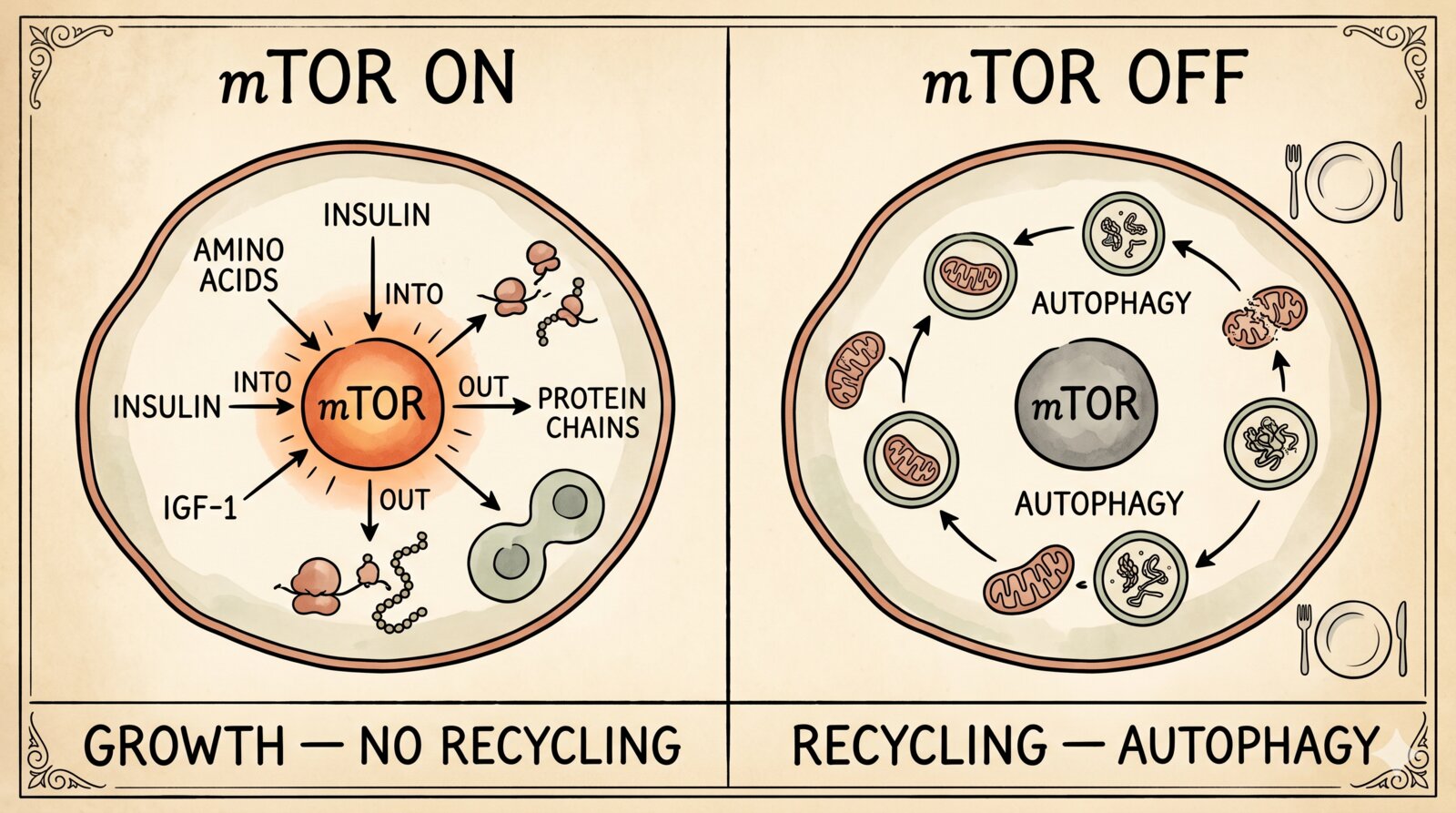
mTOR (mechanistic target of rapamycin) is a kinase that works as a cellular metabolic switchboard: it integrates signals about amino acid availability (especially leucine), insulin and growth factors (IGF-1), and cellular energy (ATP/AMP ratio). In the presence of nutrients and insulin, the mTORC1 complex is active: the cell synthesizes proteins, grows, proliferates, and switches off autophagy. When any of those inputs drops — fewer amino acids in the blood, less insulin, less energy — mTORC1 is inhibited, protein synthesis slows, autophagy reactivates, cells turn on stress-resistance programs (Saxton & Sabatini, Cell 2017 — PMID 28283069).
mTOR is one of the most studied targets in aging biology for a precise reason: animal models in which mTORC1 is inhibited — genetically or pharmacologically — live longer, develop fewer tumors, and better preserve immune and cognitive function.
The strongest animal data point isn’t about fasting: it’s about rapamycin, the pharmacological mTOR inhibitor. In the National Institute on Aging’s Interventions Testing Program (Harrison and colleagues, Nature 2009 — PMID 19587680) genetically heterogeneous mice treated with rapamycin even late in life showed a significant lifespan extension. It’s one of the few pharmacological interventions with a clean effect on murine longevity, replicated in independent labs.
In humans the picture is far more cautious. The trials by Mannick and colleagues (Science Translational Medicine 2014 — PMID 25540326; 2018 — PMID 30021824) showed that low-dose mTOR inhibitors can improve vaccine response in the elderly and reduce respiratory infection incidence — an immune outcome, not a longevity one. More recent geroscientific trials on rapamycin (PEARL, RAP-PAC) are underway, with still partial preliminary results. They aren’t enough to talk about confirmed human longevity, but the rationale holds.
Here is the point. The link between fasting and mTOR is direct and well documented — fasting lowers insulin, IGF-1, and circulating amino acids, and this reduces mTORC1 activity — but the dose and duration of the signal depend heavily on the protocol.
- Sixteen hours of overnight fasting produce an mTOR oscillation that lasts a few hours. The cell sees a small dip and goes back to anabolic mode at the first meal. It’s plausible that a benefit accumulates over time, but the per-cycle signal is small.
- Five consecutive days of FMD produce a much longer inhibition: IGF-1 drops markedly, baseline insulin stays low for days, amino acids (leucine in particular) are reduced by the low-protein protocol. The cell spends entire days in recycling and stress-resistance mode, not hours.
- Chronic rapamycin produces a constant mTORC1 inhibition, qualitatively different from both previous cases.
Claiming that 16 hours of fasting are equivalent, in molecular or longevity terms, to a rapamycin treatment is a narrative shortcut, not a data point. Claiming that the FMD comes closer to that mechanism is reasonable — with the caveat that human trials on long-term outcomes haven’t arrived yet.
In other words: mTOR is the most solid molecular rationale for which periodic fasting might count clinically more than daily fasting. It’s a rationale, not a demonstration. It’s worth knowing in order to read the promises without being swept away by them.
5. Insulin sensitivity and meal timing¶
There’s a second point on which intermittent fasting does something specific, independently of caloric deficit. The study by Sutton and colleagues (Cell Metabolism 2018 — PMID 29754952) applied an early time-restricted feeding protocol — 6-hour eating window with the last meal at 3 p.m. — to eight men with prediabetes, isocalorically. After five weeks: significant improvements in insulin sensitivity, blood pressure, oxidative stress. Without weight loss.
The principle is circadian: insulin and cortisol follow daytime rhythms, eating in the evening — when insulin sensitivity is naturally lower — is metabolically less efficient than eating in the morning.
Three caveats are needed.
- The advantage concentrates on the early versions of time-restricted eating (eat early, finish early), not on the classic 16:8 that skips breakfast and ends dinner at 9 p.m.
- The effect is documented on biomarkers; extrapolating to long-term clinical outcomes (diabetes incidence, cardiovascular events) requires longer and larger trials than those available.
- Most Italian adults practicing IF skip breakfast, not dinner. That is, they do the opposite of the protocol that shows the strongest signal.
The Sutton signal and the Wei signal on FMD speak to each other: both say that the interesting clinical target of fasting is insulin sensitivity, and that you reach it by arranging food in time (eTRE, early window) or with periodic cycles of strong restriction (FMD), much less with a generic 16:8 that just shifts the window forward without further constraints.
6. Autophagy, browning, longevity: what mice show and humans don’t¶
It’s worth holding three mechanisms together that fasting marketing cites as proof of efficacy, but which share the same problem: solid in rodents, partial in humans.
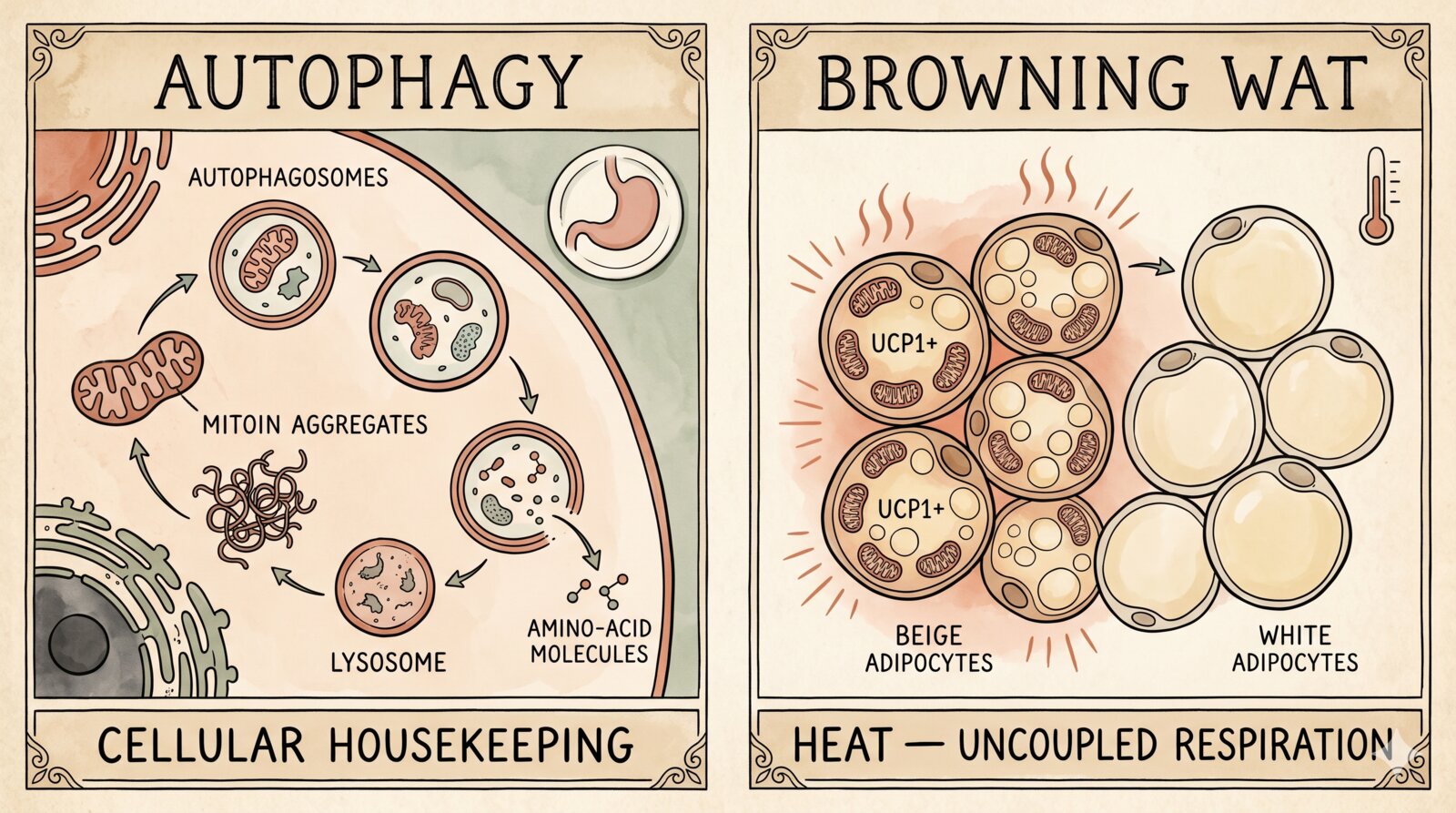
Autophagy. The process by which cells degrade and recycle damaged components. Yoshinori Ohsumi won the Nobel in 2016 for clarifying its mechanisms in yeast. In humans, measuring it in vivo is difficult (LC3, p62 in biopsies); a rise in markers doesn’t automatically mean “more cleaned-up cells”. You need prolonged fasts (≥24-48 hours) for a measurable autophagic signal to appear, not a daily 16:8. The de Cabo and Mattson review (N Engl J Med 2019 — PMID 31881139) — the most cited document in defense of fasting — is explicit about caution in extrapolating from animal models.
White adipose tissue browning. In rodents, intermittent fasting induces the appearance of UCP1+ adipocytes inside WAT, with improved glucose tolerance (Li 2017 — PMID 29107504; Kim 2017 — PMID 28959014). In humans adult BAT is quantitatively small (Cypess 2009 — PMID 19357406) and fasting-induced WAT browning is documented far more weakly, largely through indirect markers. The phenomenon exists, the clinical translation — more calories burned, a relevant weight effect via browning — is not quantified.
Longevity. Caloric restriction extends life in yeasts, worms, flies, rodents; in non-human primates the effects are smaller and context-dependent. The CALERIE trial in humans (25% caloric restriction for two years in healthy adults) showed improvements in biomarkers (insulin sensitivity, inflammation, lipid profile). Mortality benefit: impossible to measure in two years. On intermittent fasting per se in relation to human longevity, long-term data don’t exist.
The shared frame is that for almost every molecular mechanism attributed to fasting — autophagy, browning, lifespan extension — there’s a solid biological base in animals and a human replicability still to be built. Recognizing this doesn’t mean denying the phenomenon; it means proportioning the promises to the strength of the data.
7. Adherence: the real advantage of daily protocols¶
For the daily protocols — 16:8, 18:6 — there’s a point at which they do something concrete, and it’s the least spectacular point of all: for some people, they’re simply easier to follow than a classic diet.
Eating less at every meal requires thinking about food at every meal, calculating portions, saying no several times a day. Eating only in a window requires one decision a day and then no need to come back to it. For someone with a difficult relationship with food planning, it’s a real cognitive simplification.
It’s the advantage that the more recent clinical literature recognizes most solidly on daily protocols. Not a mysterious metabolic effect: a behavioral strategy that works better for some psychological profiles and worse for others. For others still, the restricted window triggers bingeing — they reach noon hungry and eat too much, too fast, without quality. For these profiles, intermittent-fasting adherence is worse, not better, than a well-structured traditional diet.
8. Who it isn’t right for¶
Part of the problem with popular communication about intermittent fasting is that it’s presented as suitable for everyone, possibly with a generic “consult your doctor”. There are precise categories for which it’s a bad idea, and it would be correct to say so out loud — it applies to all protocols, from 16:8 to FMD.
Women of fertile age, especially if athletic or underweight. Prolonged or aggressive food restriction in this group can interfere with the hypothalamic-pituitary-gonadal axis, alter the menstrual cycle, reduce fertility. The RED-S syndrome (Relative Energy Deficiency in Sport) describes exactly this picture. The signal isn’t hypothetical: evolution has wired the female body to be highly sensitive to energy availability, because reproduction requires resources, and prolonged deprivation reads as famine.
Pregnancy and breastfeeding. Never. Caloric and specific-nutrient intake (folate, iron, calcium, protein) is bound to a daily minimum that fasting would violate.
Adolescents. Caloric and energetic intake during growth is non-negotiable. Skipping meals regularly in adolescence has documented consequences on growth, bone development, cognitive performance, and is a risk factor for eating disorders.
Sarcopenic elderly. Aging reduces muscle mass and lean-mass quality. In an elderly person with sarcopenia or pre-sarcopenia, prolonged periods without distributed protein intake during the day accelerate muscle loss. For this population the recommendation is the opposite: frequent, distributed meals, with regular protein quotas.
Anyone who has or has had an eating disorder (anorexia, bulimia, binge eating). Intermittent fasting normalizes, indeed prescribes, behaviors that in these people are symptoms: skipping meals, rigid control, the fast/binge dichotomy. It’s a practice that can reactivate clinical pictures. It should be explicitly discouraged.
Type 1 diabetes and type 2 diabetes on insulin therapy. Concrete risk of hypoglycemia during fasting hours, especially if therapy isn’t readjusted. Practicable only with diabetological supervision and dose review.
People on chronic pharmacological treatment that requires intake with food. Banal, but often ignored.
This list isn’t a footnote. It’s half of the clinical conversation about intermittent fasting, and in popular marketing it’s almost absent.
9. What I’d say to someone who asks me¶
When a patient or a friend asks me whether intermittent fasting “is good for you”, the honest answer I try to give is in these lines.
If you want to lose weight, a daily protocol (16:8, 18:6) is a reasonable tool if it helps you build a caloric deficit without causing evening binges. It is not metabolically superior to a well-built classic hypocaloric diet. Don’t expect “autophagy” or “longevity” — those terms, as used on social media, are marketing, not clinic.
If you want a more solid clinical signal — better insulin sensitivity, more contained low-grade inflammation, cleaner cardiometabolic markers — the fasting-mimicking diet, done in periodic cycles (for example one a month or one every two-three months, ideally under nutritional guidance), has the most convincing scientific base. It has to be repeated over time to maintain the effect. ProLon is one convenience option but not the only one: the logic is replicable with normal food, low protein and low glycemic index, over five consecutive days.
If you’re curious about the circadian version, try an early TRE (eating window in the morning, last meal by 5-6 p.m.) for a few weeks, ideally with a metabolism already at the edge. It’s the daily protocol with the most solid signal on insulin sensitivity, but it’s not practicable for those who work late.
If you have a history of eating disorders, you’re pregnant, you’re under twenty, you’re an elderly woman with little muscle mass, or you’re on insulin therapy, leave it alone — whatever the protocol.
Expect, if anything, a small weight loss (if you eat less than your needs), a certain loosening of cognitive control over food, and — for the periodic FMD — a measurable signal on glucose, IGF-1, CRP. It isn’t little. It also isn’t the metabolic revolution they tell you about.
Closing¶
Intermittent fasting is a category too broad to judge as a block. On the daily protocols the literature has scaled back the promises: it doesn’t melt fat more than a classic diet, it doesn’t “clean up” cells in a clinically relevant way, it doesn’t extend life in a demonstrated way. For some it’s the simplest formula to follow, for others it’s the wrong one. Contraindications exist and have to be taken seriously.
The case that holds up clinically is Longo’s fasting-mimicking diet: five days a month, replicated data on insulin sensitivity and inflammation, a coherent molecular rationale via mTOR, human translation still limited to biomarkers but more solid than elsewhere. It isn’t a protocol for everyone, it isn’t a cure, and it isn’t what most intermittent-fasting books sell. It is, perhaps, the only version of “intermittent fasting” worth spending serious words on.
In nutrition, as in medicine, the interventions that actually work rarely need a book a month. They have a long history, replicated data, and a promise proportioned to them.
Essential bibliography¶
- Trepanowski JF et al. (2017). Effect of alternate-day fasting on weight loss, weight maintenance, and cardioprotection among metabolically healthy obese adults. JAMA Intern Med. PMID 28459931.
- Lowe DA et al. (2020). Effects of time-restricted eating on weight loss and other metabolic parameters in women and men with overweight and obesity (TREAT). JAMA Intern Med. PMID 32986097.
- Liu D et al. (2022). Calorie restriction with or without time-restricted eating in weight loss. N Engl J Med. PMID 35443107.
- Sutton EF et al. (2018). Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell Metab. PMID 29754952.
- de Cabo R, Mattson MP (2019). Effects of intermittent fasting on health, aging, and disease. N Engl J Med. PMID 31881139.
- Wei M et al. (2017). Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and cardiovascular disease. Sci Transl Med. PMID 28202779.
- Brandhorst S et al. (2015). A periodic diet that mimics fasting promotes multi-system regeneration, enhanced cognitive performance, and healthspan. Cell Metab. PMID 26094889.
- Saxton RA, Sabatini DM (2017). mTOR signaling in growth, metabolism, and disease. Cell. PMID 28283069.
- Harrison DE et al. (2009). Rapamycin fed late in life extends lifespan in genetically heterogeneous mice. Nature. PMID 19587680.
- Mannick JB et al. (2014). mTOR inhibition improves immune function in the elderly. Sci Transl Med. PMID 25540326.
- Mannick JB et al. (2018). TORC1 inhibition enhances immune function and reduces infections in the elderly. Sci Transl Med. PMID 30021824.
- Li G et al. (2017). Intermittent fasting promotes white adipose browning and decreases obesity by shaping the gut microbiota. Cell Metab. PMID 29107504.
- Kim KH et al. (2017). Intermittent fasting promotes adipose thermogenesis and metabolic homeostasis via VEGF-mediated alternative activation of macrophage. Cell Res. PMID 28959014.
- Cypess AM et al. (2009). Identification and importance of brown adipose tissue in adult humans. N Engl J Med. PMID 19357406.