Abstract. Aesthetic medicine is one of the medical fields where the gap between scientific evidence and advertising narrative is widest. Some treatments have thirty years of solid literature behind them; others were born yesterday and live on sponsored trials and photographic promises. Here I draw the line, one by one, between what has real clinical foundations (botulinum toxin, hyaluronic acid fillers, some lasers, peels), what has an interesting biological rationale but evidence still being built (Profhilo, polynucleotides such as Plinest, new-generation biostimulators like Ellansé and Juvelook), and what travels almost entirely on marketing (HIFU as a “lift”, injectable vitamin cocktails, mesotherapy, carboxytherapy). First of a three-part series, written for those who want to understand before they choose; the second part is Skincare: actives, concentrations and medical grade.
When you walk into an aesthetic-medicine clinic, you are usually handed a menu. Toxin, fillers, biostimulators, skinboosters, polynucleotides, injectable vitamins, next-generation lasers, scalpel-free lifts, peels, microneedling, PRP. Prices change, names change every year, the promises do not: “natural rejuvenation”, “skin quality”, “collagen stimulation”, “lifting effect”. But behind this menu — almost always presented in identical language — lies an enormous gap in scientific evidence. Some treatments have thirty years of independent literature, randomised trials, well-documented safety profiles. Others have a handful of studies, often manufacturer-sponsored, and a mechanistic rationale that sounds convincing — but is not yet clinical evidence. Others still are pure narrative, propped up by before-and-after photos and the perceived authority of whoever is offering them.
There are two mirror-image mistakes when discussing aesthetic medicine. The first is wholesale rejection — “it’s all vanity, it’s all marketing, it’s all dangerous”. This is wrong because many treatments really do work, have medical as well as aesthetic indications, and improve the quality of life of those who choose them with awareness. The second is blind enthusiasm — “if it’s new it’s better, if it costs more it’s better, if everyone is doing it, it must mean something”. This is wrong because aesthetic medicine is one of the fields where marketing innovation systematically precedes clinical innovation, and where many technologies we now consider obsolete are still on sale.
This article tries to stand in the middle. It goes through the menu’s protagonists one by one, distinguishes solid evidence from evidence-still-being-built from pure marketing, and explains — where appropriate — why a promising treatment is not yet a proven treatment.
1. What we mean by “it works”¶
Before getting into individual treatments, it is worth nailing down what “it works” means. At least three levels of evidence circulate in aesthetic medicine, often conflated:
Mechanistic plausibility. “This molecule activates fibroblasts, therefore it stimulates collagen.” That is a hypothesis, not a conclusion. Plenty of molecules activate fibroblasts in vitro without producing any visible benefit on human skin. Plausibility is a starting point, not an arrival point.
Preclinical evidence. Studies on cell cultures, on ex-vivo tissues, on animal models. Useful for working out whether a hypothesis is worth testing in humans. They never replace clinical trials.
Clinical evidence. Studies on real people, ideally randomised, controlled, adequately sized, with sufficient follow-up and measurable outcomes (not just “patient satisfaction”). This is the level that counts. It is also the rarest level in aesthetic-medicine marketing.
To these you have to add an implicit but decisive criterion: who funds the study. A manufacturer-sponsored trial is not automatically false, but it carries a systematic risk of positive outcomes. When the only literature on a treatment is industry-funded, read it with proportionate caution.
With this grid in mind, let’s see what is actually on the table.
2. Botulinum toxin: the gold standard¶
Type-A botulinum toxin (Botox, Azzalure, Bocouture, Xeomin, Dysport) is the most-studied treatment in aesthetic medicine. It has been used medically since the eighties — first for strabismus, then for blepharospasm, dystonia, chronic headache, hyperhidrosis — and cosmetically since 2002, the year the FDA approved its first cosmetic indication (glabellar lines).
The mechanism is well defined: the toxin temporarily blocks the release of acetylcholine from motor nerve terminals, paralysing the target muscle for about three to four months. Dynamic wrinkles — the ones that appear with muscle contraction (forehead, glabellar, crow’s feet) — soften because the muscle no longer contracts. Static wrinkles, sculpted into the skin over time, soften less, or not at all.
The evidence is massive. Hundreds of independent randomised trials, decades of pharmacovigilance, a well-documented safety profile at cosmetic doses. Complications exist — eyelid ptosis, asymmetry, “frozen” expressions — but they are almost always dose-dependent and operator-dependent, and resolve as the toxin is metabolised.
There is a second level of effectiveness, less talked about by marketing but very useful in clinical practice, which has to do with the balance between the elevator and depressor muscles of the face. The muscles of facial expression are roughly organised into two families: the elevators, which pull tissues upwards (zygomaticus, levator labii superioris, frontalis), and the depressors, which pull them downwards (depressor anguli oris — DAO —, platysma, depressor labii inferioris, mentalis). With age the balance shifts in favour of the depressors: the muscles that pull downwards relatively “strengthen”, while the support of the elevators wanes through loss of tone and volume. It is one of the biomechanical reasons why the corners of the mouth turn downwards, the chin tightens, the neck loses definition.
Botulinum toxin can modulate precisely this imbalance. Selectively injected into the depressors — the classic example is the DAO to redraw the corner of the mouth, or the platysma for the so-called “Nefertiti lift” of the jawline — it produces a relaxation that lets the elevators act undisturbed. The result is a small but real “functional lift”: not a true volume reconstruction, not a change to the face’s architecture, but a correction of the muscular traction vector. It is one of the indications where toxin, beyond dynamic forehead and glabellar wrinkles, shows its value with greatest elegance — and it requires an operator with a precise map of each individual patient’s facial-expression anatomy, because injecting the wrong depressor, or the wrong muscular plane, produces obvious asymmetries.
The real limit remains a single one: toxin works on muscles, not on skin quality, volume, tissue laxity. When it is sold as “global rejuvenation” you have stepped outside the perimeter of the evidence. It works very well for what it has been approved and validated for — both on dynamic wrinkles and on elevator/depressor balance. Full stop.
3. Hyaluronic acid fillers: solid but often misunderstood¶
Injectable hyaluronic acid (Restylane, Juvéderm, Belotero, Aliaxin, Teosyal, Princess) is the second pillar of aesthetic medicine. It is a polysaccharide naturally present in the skin, produced industrially by bacterial fermentation and then chemically cross-linked to obtain gels of varying consistency, from the most fluid (for lips and fine lines) to the densest (for cheekbones, chin, volume reconstruction).
The evidence is solid for the codified uses: volume restoration (cheekbones, temples, chin, jawline), augmentation or redefinition of the lips, correction of nasolabial folds and the so-called “marionette lines”. It works, it is reversible (hyaluronidase degrades the gel if anything goes wrong), and it has a reasonable safety profile in experienced hands.
The problems with filler are not in the filler. They are in three phenomena that marketing would rather not discuss:
Migration and accumulation. Cross-linked fillers persist in the tissues longer than the “12–18 months” promise suggests. MRI studies have shown visible residue even five years after the last injection, along with migration of the product to sites other than the injection point (cheekbones drifting under the eyes, lips spreading above the vermilion border). The problem worsens with repeated injections over time.
Cumulative effect and pillow face. Anyone who redoes their filler every twelve months for years accumulates product. The face loses its natural geometry, the cheekbones flatten into broad surfaces, the lips become disproportionate. The phenomenon is so common that it has its own name (“pillow face”, “filler face”) and is visible in a great many middle-aged celebrities.
Vascular complications. Rare but serious: occlusion of an artery with cutaneous necrosis, and — in extreme cases — retrobulbar embolisation with blindness. They are operator-dependent, and they are what marks the difference between a doctor who knows the vascular anatomy of the face and an improvised operator.
Hyaluronic acid filler is not marketing: it is a real medical treatment, with real indications. The problem is almost always in the excess, and in the hand wielding it.
4. Classical biostimulators: Sculptra, Radiesse¶
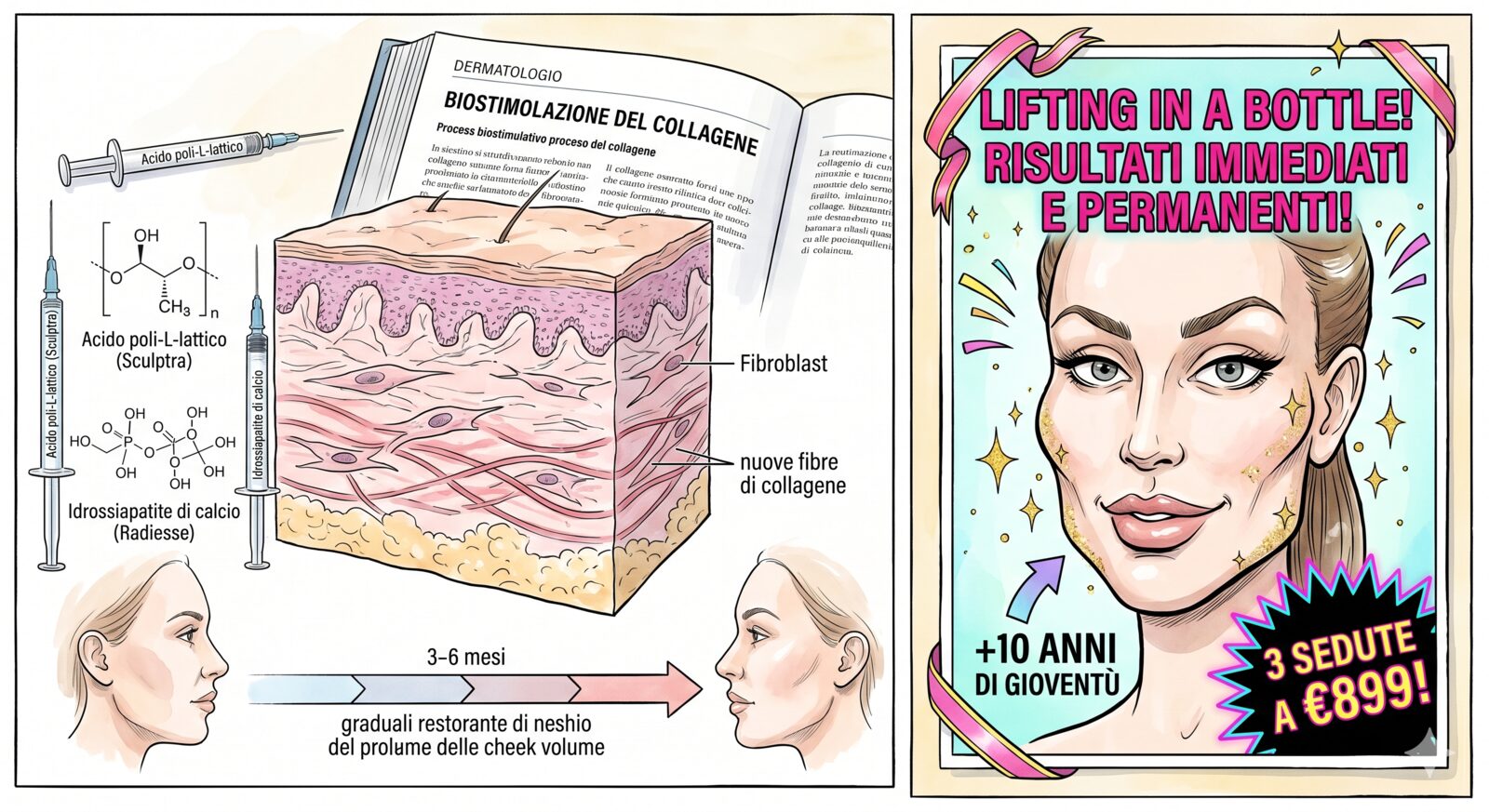
A different category from traditional fillers. Biostimulators do not fill directly — or only minimally — but stimulate tissue to produce its own collagen. Volume builds up over time, weeks or months after injection, and lasts longer.
Sculptra (poly-L-lactic acid, PLLA). Microparticles of a biodegradable polymer suspended in aqueous solution. Injected deep, PLLA stimulates a fibroblastic response with new production of type-I collagen. The evidence is decent, with randomised trials (some of them independent) for the correction of HIV-associated lipoatrophy — its original indication, later extended to aesthetics. Duration is 18–24 months. Limit: it requires several spaced sessions, the effect demands patience, and subcutaneous nodules are not an uncommon complication, especially if the operator fails to massage the area adequately or injects too superficially.
Radiesse (calcium hydroxylapatite, CaHA). Microspheres of hydroxylapatite — the same molecule as bone — suspended in a carrier gel. Dual mechanism: immediate filling from the gel + collagen stimulation from the microspheres as they degrade. FDA-approved, with good evidence for the codified indications (hands, jawline, sub-platysmal areas). Duration 12–15 months. Limit: it is not reversible (there is no “hyaluronidase” for calcium hydroxylapatite), and in superficial areas it can leave visible whitish nodules.
Both have solid clinical foundations. Recent marketing is repositioning them as “skin-quality boosters” for superficial injection, an indication far less studied and with more risk of complications. Used for what they were validated for, they work.
5. The new generation: Ellansé, Juvelook and the hybrids¶
In recent years a category has exploded that marketing calls “next-generation biostimulators” or “hybrid fillers”. These are products that combine an immediate filling effect (HA or carrier gel) with a slower biostimulating effect (polymeric microspheres).

Ellansé (PCL — polycaprolactone). Microspheres of polycaprolactone in a carboxymethylcellulose gel. Four formulations with progressive duration (S, M, L, E — 12, 18, 24, 36 months as declared). It carries a CE mark in Europe but no FDA approval in the United States — a detail worth keeping in mind. The evidence is decent, with some respectable trials for deep volumes and the correction of HA-resistant areas. The flip side is serious: more demanding complications than HA fillers (nodules, granulomas, late inflammatory reactions) and no reversibility — there is no enzyme that degrades injected polycaprolactone. If it goes wrong, it goes wrong.
Juvelook (PDLLA + HA). Korean, a hybrid of poly-D,L-lactic acid microspheres and non-cross-linked hyaluronic acid. Designed for superficial use as a “skinbooster with biostimulation”. The rationale is reasonable — PDLLA is a cousin of Sculptra’s PLLA, well characterised — but the aesthetic evidence is almost all Korean, drawn from small, often industry-funded trials. We are in the “promising, not yet sufficiently validated” phase.
Lenisna, Gouri, and the others. A flood of similar products is arriving from the Asian market, each with its own polymer (PDLLA, PCL, PLA in various forms) and its own carrier gel. Many have a CE mark, few have independent trials published in mainstream journals.
The strategic mistake here is to assume that “new” means “better”. The advantage of an Ellansé over a Sculptra, or of a Juvelook over a classic skinbooster, has to be demonstrated — not assumed because the company says so. For patients with good skin and preserved volumes, the most-studied and reversible products (good-quality cross-linked HA) are often the most rational choice. For those with real needs for deep volume and extended duration, the classical biostimulators (Sculptra, Radiesse) have decades of literature behind them. The new generation should be reserved for those who have understood that they are choosing a product with less data and less reversibility in exchange for fresher marketing.
6. Profhilo and the bioremodellers: a promising area, not yet a gold standard¶
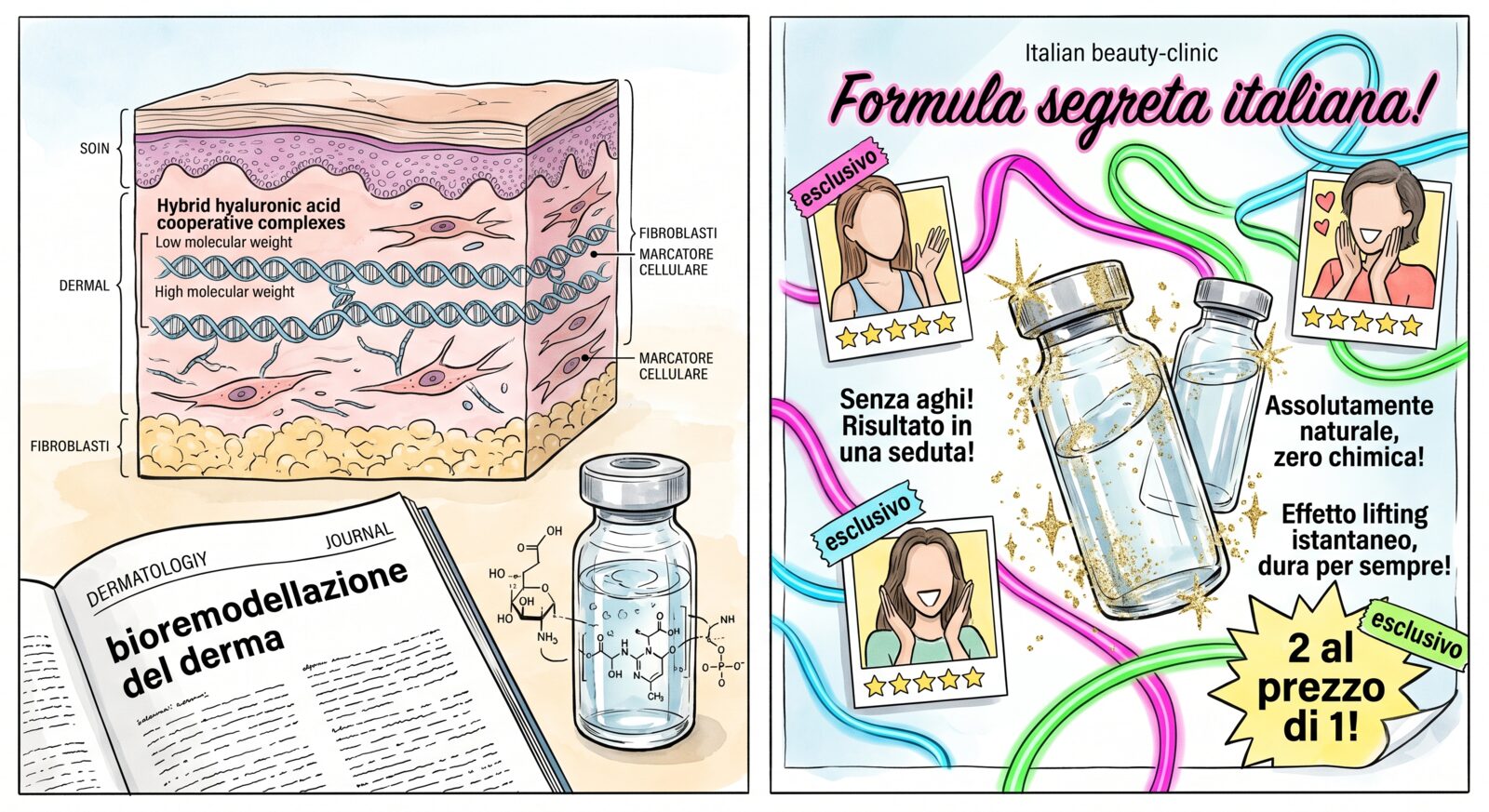
Profhilo (IBSA). Thermally stabilised hyaluronic acid (NAHYCO technology), not chemically cross-linked, of very high molecular weight. Technically it is not a filler — it does not fill volumes — and it is sold as a “bioremodeller” for lax skin on the face, neck, arms, hands, abdomen.
The proposed mechanism is a slow release of HA that hydrates tissues and stimulates fibroblasts to produce collagen and elastin. The evidence is decent and growing. Histological studies document actual dermal remodelling after sessions, and clinical trials with instrumental outcomes (cutaneous ultrasound, elastometry) show measurable changes.
The honest limit is twofold. First, almost all the published RCTs are sponsored by IBSA — the manufacturer — and independent trials are few, small, with heterogeneous methodologies. Second, the “rejuvenation” claim marketing leans on needs scaling down: the real effect is deep skin hydration and a slight recovery of tone, not a lift or volumetric remodelling. It works, but on a more modest scale than the brand names suggest.
The same reasoning applies to the family of “bioremodellers” and new-generation “skinboosters” (Viscoderm Hydrobooster, Restylane Skinboosters, Belotero Revive, Hydro Deluxe). All are hyaluronic acids of varying density, designed to improve the hydration and superficial quality of the skin. The evidence varies from product to product; the active ingredient is essentially the same, the stabilisation technologies differ — but the efficacy gap from one brand to another is probably smaller than the price lists would have you believe.
A separate note for Volite (Juvéderm/Allergan), a medium-density non-cross-linked HA marketed both for skin quality and — increasingly — for atrophic post-acne scars. On skin quality the evidence is in line with the rest of the family: measurable but modest gains in hydration and luminosity, with the usual caveat that the trials are almost all industry-funded. On scarring, however, the rationale is weak: HA does not durably fill volume in fibrotic tissue and does not induce neocollagenesis comparable to microneedling, fractional lasers, or polynucleotides. It is an indication heavily pushed by marketing, but for atrophic scars the more solid choices lie elsewhere. I will dedicate a separate article to scarring: it deserves more space than a paragraph.
7. Polynucleotides: solid rationale, aesthetic evidence under construction¶

One of the best-selling categories in Italy in recent years. Polynucleotides (PDRN — polydeoxyribonucleotides; PN-HPT — polynucleotides of very high molecular weight) are DNA fragments extracted from the gonads of trout or salmon, purified and injected for therapeutic purposes. The most widespread brand names are Plinest, Newest, Mastelli, Rejuran (Korean).
The proposed mechanism is interesting: the DNA fragments bind A2A adenosine receptors, activating anti-inflammatory and proliferative signals on fibroblasts. The biological rationale is far more solid than that of many other categories — it is not “stimulates collagen” thrown around loosely, it is a plausible and partly characterised mechanistic chain.
The strong evidence sits in other fields: healing of chronic wounds, venous and diabetic ulcers, and — with intra-articular use — osteoarthritis. In these contexts PDRN has decent trials and consolidated clinical indications.
The aesthetic evidence is thinner. Small-scale trials, mostly Korean and Italian, often industry-funded, with heterogeneous outcomes. The most solid claims concern skin quality, dark under-eye circles, scarring, sun-damaged skin. The weakest claims concern generic “rejuvenation” and non-surgical lifting — claims the product, by virtue of how it works, simply cannot sustain.
Honest positioning: polynucleotides are one of the more interesting treatments of the coming years, with a biological rationale worth following. But we are in the phase where the promise precedes the data. For anyone who chooses to have them, it is reasonable to do so knowing that the evidence is still being built, not settled.
8. Injectable vitamins and mesotherapy cocktails¶
Here the discussion forks. Under the generic label “injectable vitamins” or “skinboosters” two different families actually live, with very distant scientific statuses.
Family 1: pure or near-pure non-cross-linked HA. Profhilo (already covered), Viscoderm Hydrobooster, Restylane Skinboosters Vital, Belotero Revive. These are hyaluronic acids of varying density, with at most a minimal addition of other molecules (glycerol, mannitol). The evidence is what we discussed above: decent, mostly industry-funded, with real but more modest effects than advertised.
Family 2: multi-ingredient cocktails. NCTF 135HA (Filorga, now part of the Colgate-Palmolive group), Dermaheal, BCN cocktails, and a myriad of mesotherapy formulations. They typically contain non-cross-linked HA + 50–60 other ingredients: vitamins (A, B, C, E), amino acids, coenzymes, minerals, antioxidants. The marketing is heavy and the rhetorical move is always the same: “nourishes skin from within”.
The scientific problem is that those 50–60 ingredients have no evidence of clinical efficacy when injected into the dermis at the concentrations and volumes used. The trials published on NCTF 135HA, for example, are overwhelmingly Filorga-sponsored, with soft outcomes (patient self-assessment, standardised but non-blinded photographs) and weak or absent control groups. The HA part does something — that is biochemical fact — but the difference between injecting pure HA and injecting HA + 53 other things has not been demonstrated.
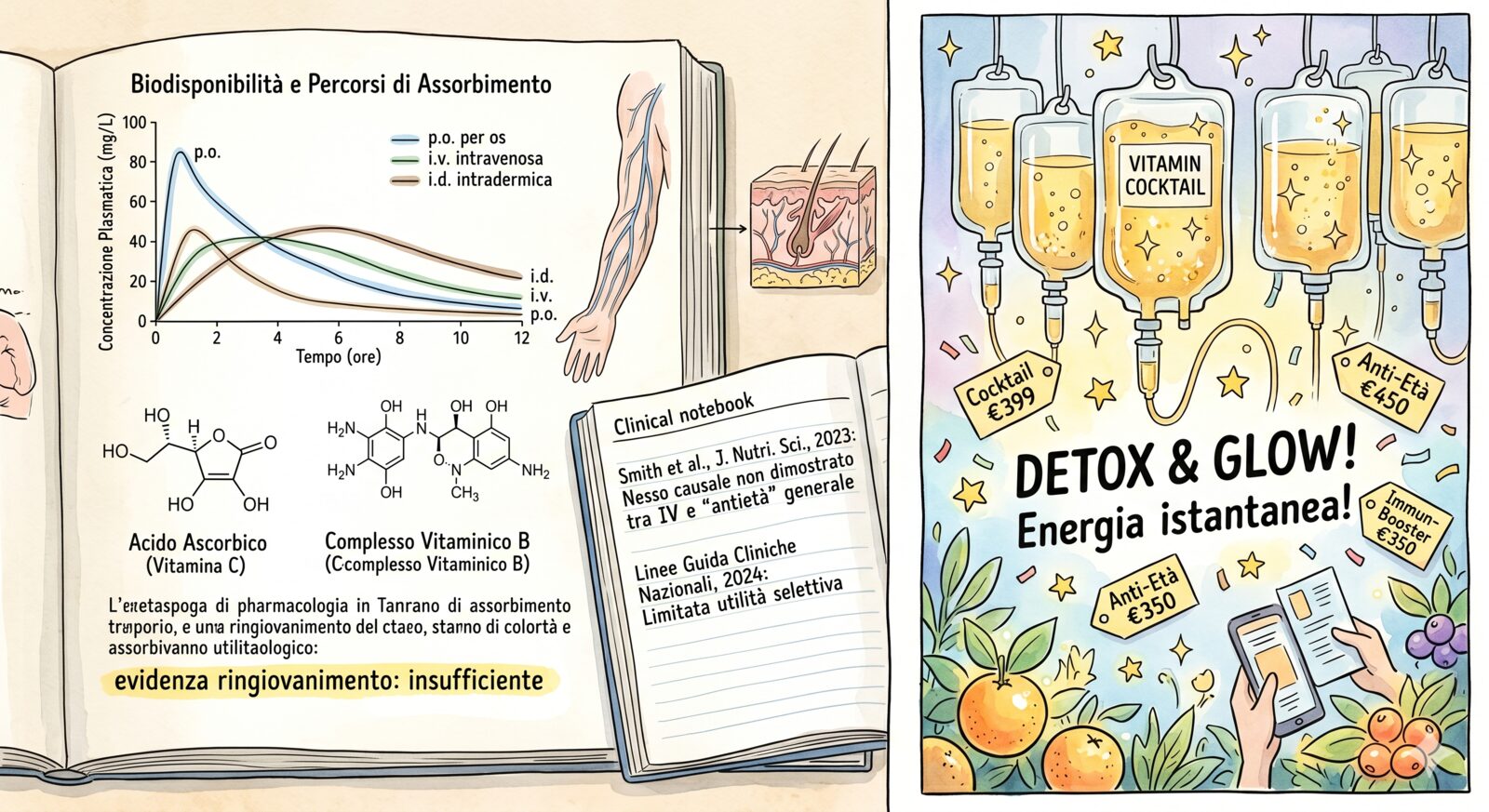
There is also a simpler pharmacological consideration. Vitamins administered orally or intramuscularly have known pharmacokinetics and sometimes real clinical indications. Those same vitamins injected into the dermis at micro-doses — below any pharmacologically significant threshold — fall into the territory of failed plausibility: there is no solid biochemical reason to think they exert any meaningful systemic or local effect.
Distinguishing these two worlds matters. HA-only has solid foundations. Injectable vitamin cocktails have solid marketing. They are not the same thing.
9. Energy: lasers, IPL, LED, radiofrequency, HIFU¶
A vast and uneven category. Loosely grouped under “energy-based treatments”, it actually comprises devices with very different mechanisms and very different levels of evidence.
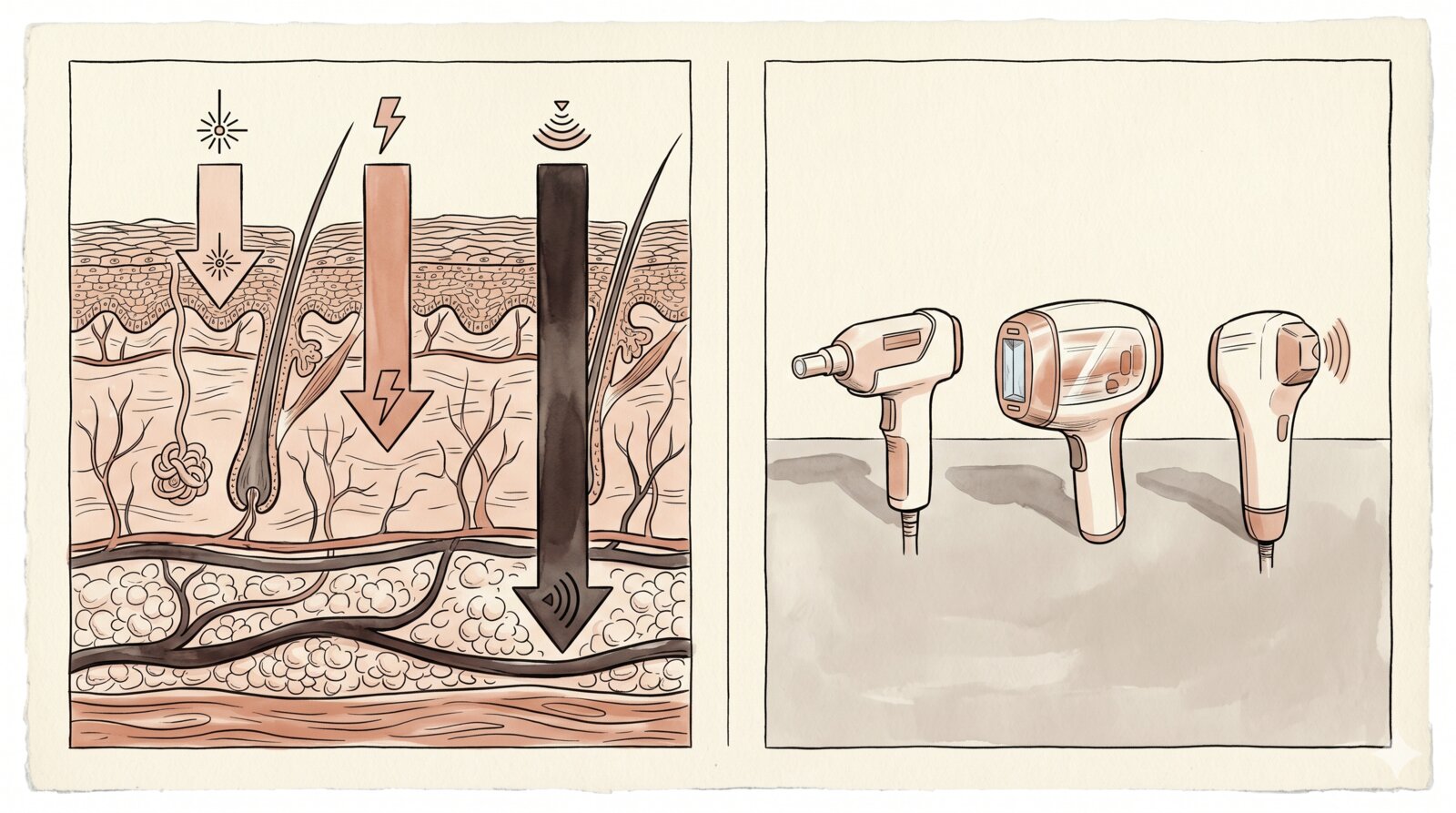
Ablative fractional lasers (CO2, Er:YAG). They destroy microcolumns of cutaneous tissue, triggering a repair response with neocollagenesis. Solid evidence for photoageing, acne scars, sun damage, surface irregularities. They are the most studied energy-based treatments, with independent randomised trials and decades of literature. Limit: long recovery times (days of erythema, desquamation, no sun exposure), and on darker skin a significant risk of post-inflammatory hyperpigmentation. An experienced operator and careful patient selection are crucial.
Non-ablative fractional lasers (Nd:YAG, Erbium glass, Thulium). Gentler effect, quick recovery, but more limited efficacy. Multiple sessions are needed. Decent for skin quality and mild photoageing.
IPL (Intense Pulsed Light). Not a laser but a filtered polychromatic light. Solid evidence for superficial pigmentations (lentigines, actinic damage) and rosacea (vascular component). Useless or risky on darker skin. An entry-level treatment heavily exploited by marketing because it is fast and cheap, but with precise indications — not “global rejuvenation”.
Red light and LED (photobiomodulation). Non-coherent light at 630–660 nm (red) and 810–850 nm (near-infrared), delivered at low power onto the skin. Mechanism: absorption by mitochondrial cytochromes, modulation of ATP production and oxidative stress, downstream effects on inflammation and fibroblast activity. Indications with reasonable evidence are inflammatory acne (combined blue + red protocols, some FDA-cleared devices), mild photoageing (measurable but small effects on fine lines and skin quality), wound healing, and androgenetic alopecia in the low-level laser/LED variant. Indications that are weak or unsupported: significant skin laxity, “lifting”, marked dyschromia. It is a low-risk, low-cost device that works if taken for what it is — an adjunct treatment with real but modest effects — not as a substitute for lasers, peels, or microneedling. The marketing of consumer devices (at-home LED masks, “anti-ageing in 10 minutes” claims) overpromises; medical devices with standardised parameters are a different story.
Monopolar/bipolar/multipolar radiofrequency. Heats deep tissues with the promise of stimulating collagen and producing tightening. The evidence is mediocre. Published trials show modest, heterogeneous effects, rarely compared head-to-head with other technologies. The commercial platforms (Thermage, Exilis, Venus Legacy) have similar claims and similar data — plenty of patient satisfaction, little objective difference. It works better as an adjuvant than as a primary treatment.
HIFU (High-Intensity Focused Ultrasound — Ultherapy, Ulfit, Liftera). Aggressive sales pitch: “scalpel-free lift”. Proposed mechanism: delivery of focused ultrasonic energy at precise depths (3–4.5 mm), to heat the SMAS (the superficial musculo-aponeurotic layer) and induce tightening. The premise is interesting; the actual clinical results are far more modest than the promises. Independent meta-analyses show small effects, highly variable across studies, rarely compared with placebo or other technologies. The word “lift” applied to HIFU is a lexical abuse: a surgical lift redraws the architecture of the face; HIFU produces — when it goes well — a modest tightening effect.
The general principle: the energy-based treatments with the most evidence are the most aggressive (ablative lasers). The ones with the least evidence are the “softest” and the most marketable as “no downtime, no pain”. It is a correlation marketing systematically inverts.
10. Chemical peels and microneedling: the underrated classics¶
Chemical peels. Acids applied to the skin at various depths to remove cutaneous layers and stimulate renewal. A category with solid evidence and almost a century of clinical use: glycolic, salicylic, trichloroacetic (TCA), Jessner, phenol (now rarely used because of how aggressive it is). Indications: dyschromia, photoageing, superficial acne scars, tissue quality. It is not marketing: it is traditional dermatology that works, at low cost, with few side effects and a vast literature behind it.
The peel is one of the treatments that recent marketing tends to snub because it is not very “technological” and not very profitable. But for a great many indications — especially chromatic and textural — a course of well-done peels is more effective, and less expensive, than many new-generation energy-based treatments.
Microneedling (dermapen, dermaroller, microneedling with radiofrequency). Microneedles that induce controlled microtraumas to stimulate cutaneous repair. Decent evidence for acne scars, stretch marks, skin quality. The radiofrequency variant (Morpheus8, INTRAcel) adds thermal delivery, which some trials show to be superior to plain microneedling, although direct comparisons are still few. It is a treatment that works, especially in courses, and it has a good efficacy-to-cost ratio.
When aesthetic medicine chooses the sensational over the solid, peels and microneedling are often the first casualties — not because they don’t work, but because they don’t sell well.
11. Mesotherapy, carboxytherapy, PRP: the grey zone¶
Three heavily sold treatments, three problematic evidence profiles.
Mesotherapy. An umbrella term for intradermal injections of variable cocktails: vitamins, amino acids, homeopathics, phytoextracts. Born in France for chronic pain, then rebranded for aesthetics. The evidence for aesthetic indications (cellulite, localised fat loss, “rejuvenation”) is almost entirely absent. Systematic reviews regularly conclude that the available studies are of low quality, heterogeneous, and do not support the claims. It is not dangerous when done well, but the cost-to-efficacy ratio is close to zero.
Carboxytherapy. Injection of medical carbon dioxide into tissues, with the promise of improving microcirculation and stimulating collagen. Limited literature, modest quality, small measured effects. The better-supported indications (stretch marks, dark circles, peripheral microcirculation) have evidence sufficient not to discard the treatment entirely, but not enough to place it among first-choice options.
PRP (Platelet-Rich Plasma) — the “vampire facial”. Blood is drawn from the patient, centrifuged to concentrate the platelets, and the platelet plasma is re-injected into the dermis or onto the skin (sometimes combined with microneedling). Rationale: platelet growth factors stimulate tissue repair. The evidence is mixed: some trials show modest benefits for skin quality and androgenetic alopecia, others show no difference compared with placebo. The regulatory problem is a separate matter: lack of standardisation in preparations and — most seriously — documented episodes of infection transmission (HIV, hepatitis C) in US clinics that reused materials. Done well, it can have its indications; done badly, it is one of the potentially riskiest treatments on the aesthetic menu.
12. How to recognise marketing¶
By the end of this list a pattern emerges. The treatments with the most aggressive marketing are often those with the least evidence; the treatments with the most solid evidence are often the most technical and the least spectacular to talk about. A few useful signals to orient yourself:
-
If “anti-ageing” is the main claim, you are probably looking at a treatment that works less well than it is sold. Serious medicine does not talk about “anti-ageing”; it talks about precise indications.
-
If the only literature cited comes from the manufacturer, read the product as a commercial hypothesis, not as evidence.
-
If the treatment promises to “stimulate collagen” but does not specify by what mechanism, in which cutaneous layer, with what histological evidence, it is almost always a marketing claim.
-
If the operator talks about “latest-generation technology” without naming the independent trials, translate: there are none.
-
If the promise is a “scalpel-free lift”, you are not getting a lift. You are getting a treatment that produces a modest effect — of tone or hydration — that marketing has rebranded.
-
If the only evaluation parameter is the before-and-after photo, remember that lighting, angle, expression and post-production change the visual result far more than the treatment does.
-
If price is the main argument for authority — “it’s expensive because it’s the best” — you are not buying efficacy, you are buying positioning.
Closing¶
Aesthetic medicine is not a scam, and it is not a panacea. It is a medical discipline with a core of serious treatments (toxin, HA fillers, classical biostimulators, ablative lasers, peels, microneedling), a ring of promising treatments whose evidence is still being built (Profhilo and bioremodellers, polynucleotides, new-generation biostimulators), and a wide periphery of treatments that are more marketing than medicine (HIFU as a “lift”, injectable vitamin cocktails, mesotherapy, carboxytherapy, some PRP variants).
The problem is not that effective treatments don’t exist. The problem is that they are all sold in the same language, and whoever chooses rarely has the tools to tell an independent randomised trial from a corporate brochure. That is why, before sitting down in an aesthetic-medicine chair, it is worth doing what you would do for any other medical decision: ask what evidence supports the treatment, who funded it, what complications are documented, how reversible it is, and what happens if it doesn’t work.
In the next two parts of this series we’ll move from the chair to the mirror: everyday skincare, and the real difference between over-the-counter and medical grade products. Because many of the problems that drive people into the clinic could be eased — or avoided altogether — with an honest routine, made of a few right actives at the right concentrations.
And because, in the end, the marketing of aesthetic medicine and the marketing of cosmetics are the same marketing. Only the needles change.
Essential bibliography¶
A handful of references, chosen to cover the most contestable claims in the article: the clinical origin of cosmetic toxin, the actual persistence of hyaluronic acid fillers on MRI, vascular complications, the rationale of polynucleotides, the HIV-lipoatrophy origin of PLLA, the NAHYCO mechanism of Profhilo, the quality of the evidence for HIFU and PRP.
- Carruthers JD, Carruthers JA. Treatment of glabellar frown lines with C. botulinum-A exotoxin. J Dermatol Surg Oncol. 1992;18(1):17-21. PMID: 1740562
- Master M, Roberts S. Long-term MRI Follow-up of Hyaluronic Acid Dermal Filler. Plast Reconstr Surg Glob Open. 2022;10(4):e4252. PMID: 35433153
- Beleznay K, Carruthers JDA, Humphrey S, Carruthers A, Jones D. Update on Avoiding and Treating Blindness From Fillers: A Recent Review of the World Literature. Aesthet Surg J. 2019;39(6):662-674. PMID: 30805636
- Valantin MA, Aubron-Olivier C, Ghosn J, et al. Polylactic acid implants (New-Fill) to correct facial lipoatrophy in HIV-infected patients: results of the open-label study VEGA. AIDS. 2003;17(17):2471-2477. PMID: 14600518
- Stellavato A, Corsuto L, D’Agostino A, et al. Hyaluronan Hybrid Cooperative Complexes as a Novel Frontier for Cellular Bioprocesses Re-Activation. PLoS One. 2016;11(10):e0163510. PMID: 27723763
- Galeano M, Pallio G, Irrera N, et al. Polydeoxyribonucleotide: A Promising Biological Platform to Accelerate Impaired Skin Wound Healing. Pharmaceuticals (Basel). 2021;14(11):1103. PMID: 34832885
- Contini M, Hollander MHJ, Vissink A, Schepers RH, Jansma J, Schortinghuis J. A Systematic Review of the Efficacy of Microfocused Ultrasound for Facial Skin Tightening. Int J Environ Res Public Health. 2023;20(2):1522. PMID: 36674277
- Maisel-Campbell AL, Ismail A, Reynolds KA, et al. A systematic review of the safety and effectiveness of platelet-rich plasma (PRP) for skin aging. Arch Dermatol Res. 2020;312(5):301-315. PMID: 31628542