Abstract. Almost all mass-market skincare is under-dosed, unstable, or poorly formulated. Almost all medical grade skincare costs more — but not always for the right reasons. Here I draw the line on what “active” really means in a cosmetic (concentration, pH, vehicle, penetration, stability), which pillars of the dermatological literature actually hold up (retinoids, vitamin C as L-ascorbic acid, niacinamide, azelaic acid, AHA/BHA), and which are the more recent fashions selling mostly stand-in ingredients: cosmetic peptides, bakuchiol as “natural retinol”, snail mucin, plant stem cells. And why — beyond a certain marketing premium — medical grade products often have technical reasons to cost more. Second part of a three-part series, after Aesthetic medicine: what works, what is marketing.
In the cosmetics aisle of a pharmacy or in the pages of a skincare e-commerce site, ingredients turn up everywhere. Vitamin C, retinol, peptides, hyaluronic acid, niacinamide, ceramides, plant oils, botanical extracts. The promise is always the same — younger, firmer, brighter, more protected skin — and the vocabulary is almost identical between an eight-euro serum and a hundred-and-twenty-euro cream.
There is a problem, and it is hard to fit on a label. A cosmetic works — when it does work — because it contains a sufficient amount of a molecule with proven efficacy, formulated so that it stays stable, and delivered so that it crosses the stratum corneum enough to do something. Almost the entire mass-market skincare industry trades on the perception of efficacy — pleasant texture, fragrance, bottle design, marketing claims — more than on actual efficacy. It is not a scam: it is a sector with an enormous grey area between “contains an active ingredient” and “does what it promises”.
This article tries to make that grey area a little less grey. It distinguishes what “active” really means, separates the major pillars from the fashions, explains how medical grade actually differs from the mass market, and also points out where the difference is purely commercial positioning.
1. What “active” means: the four variables that count¶
Before talking about individual molecules, it is worth setting out the principle. An active molecule, on its own, is not enough. Whether a cosmetic works depends on at least four intertwined variables:
Concentration. Almost every active has a minimum threshold below which it produces no detectable effect. For tretinoin (the pharmaceutical retinoid) we are talking 0.025-0.1%. For vitamin C as L-ascorbic acid, 10-20%. For niacinamide, 4-10%. Below those thresholds the ingredient is “present” but essentially decorative. European cosmetic regulation requires ingredients to be listed in decreasing order of concentration — but not to declare the actual amount — and almost the entire mass market exploits that grey area to boast ingredients that are present only in traces.
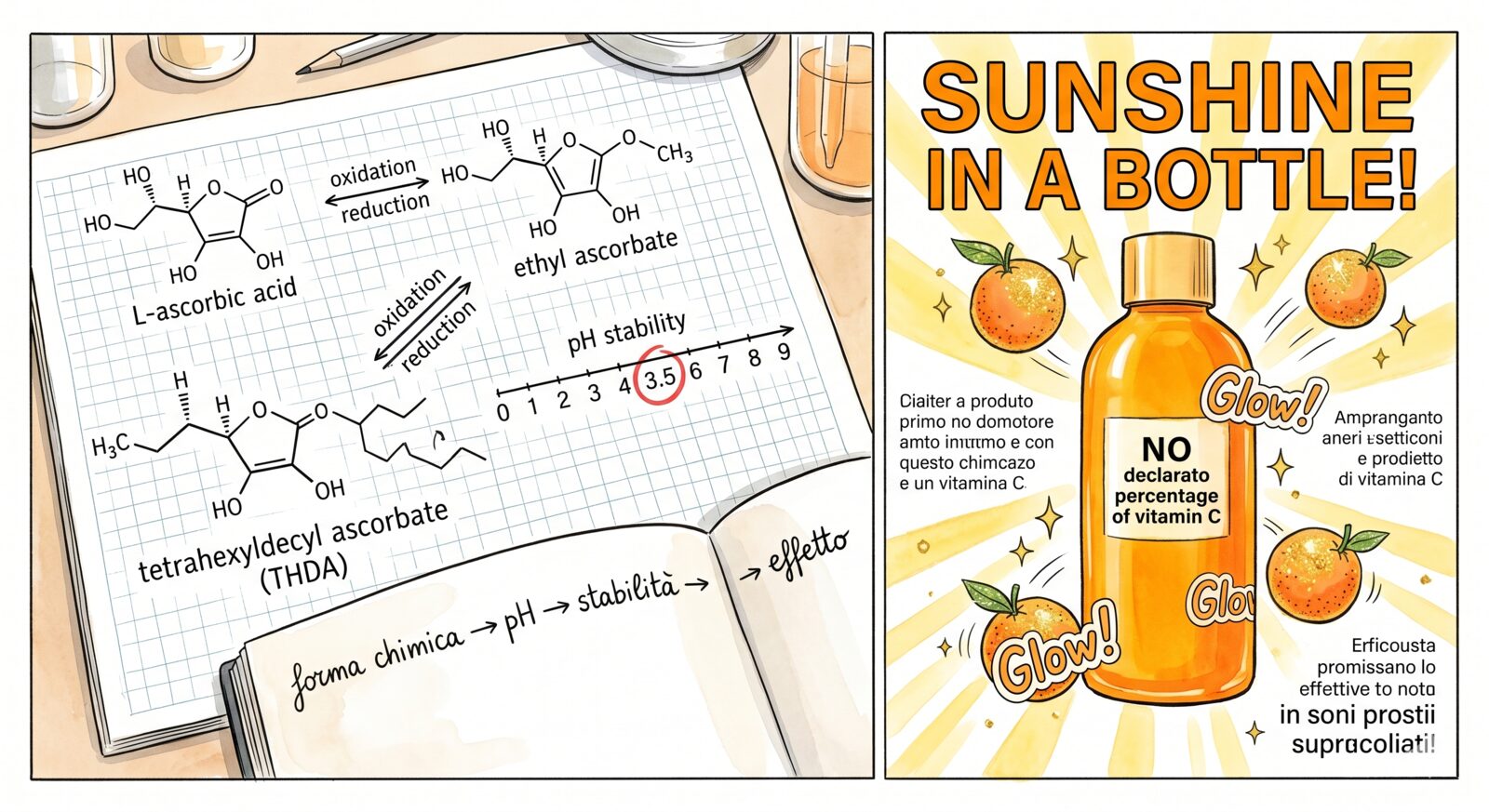
pH. Many actives behave differently at different pH values. L-ascorbic acid is only effective below pH 3.5; above that, it neither penetrates nor stays stable. AHAs work in the 3-4 range. Niacinamide tolerates a wider window. A formulation at the wrong pH cancels the efficacy even if the concentration is right.
Stability. Some actives oxidise or degrade rapidly on contact with air, light, or heat. Vitamin C in aqueous solution turns yellow and then brown as it oxidises — and once oxidised it no longer works; in fact, it can even promote oxidative stress. Retinoids are photosensitive. The packaging (airless bottles, dark glass, single-dose capsules) and the formulation (co-antioxidants, more stable derivatives) determine whether the product you paid for will still work after three months in the bathroom drawer.
Vehicle and penetration. The stratum corneum is a barrier designed to let almost nothing through. Many actives have to cross it to work. The difference between a formulation that penetrates and one that sits on the surface can come down to emulsifiers, lipids, carriers (liposomes, microencapsulation), or derivatives specifically designed to cross the barrier (retinaldehyde vs retinyl palmitate, ascorbyl glucoside vs L-ascorbic acid).
Four variables, any one of which can make a product effective or useless. When a brand advertises “with vitamin C” without declaring the chemical form, the concentration, the pH, and the stabilisation system, it is selling the ingredient, not the effect.
2. Why the mass market is almost always under-dosed¶
The mass-market cosmetic industry works under constraints that dermatology does not. A product must be:
- Tolerable by an enormous and heterogeneous population, including sensitive skins that have never used an active. Hence concentrations are often calibrated downward.
- Stable for 24-36 months on the shelf. Hence the more potent (and more unstable) chemical forms are often replaced with derivatives that keep better but work less.
- Fragranced and pleasant to the touch, because skincare is a sensory experience before it is a pharmacological one. Added perfumes and essential oils raise the risk of allergic reactions and irritation.
- Priced in a way that allows significant margins on distribution, marketing, and packaging. The raw material is often a tiny fraction of the final cost.
The result is predictable. A supermarket vitamin C serum typically contains 0.5-2% of a stable derivative (ascorbyl glucoside, magnesium ascorbyl phosphate), well below the documented efficacy threshold. A “retinol” cream often contains retinyl palmitate, a form with negligible clinical efficacy compared with retinol or retinaldehyde. A “with peptides” formulation typically contains peptide chains at concentrations on the order of 0.1%, well below any documented biological effect.
It is not that mass-market products never work. Moisturisers, occlusives, and good-quality physical and chemical sunscreens are available at accessible prices and do their job. But when the product promises an active effect — anti-ageing, anti-spot, brightening, stimulating — the probability that it delivers scales with concentration and formulation, not with the list price.
3. Retinoids: the gold standard, and its cousins¶
Retinoids are the class of actives with the most robust evidence in all of cosmetic dermatology. Decades of literature, independent randomised trials, a well-characterised cellular mechanism.
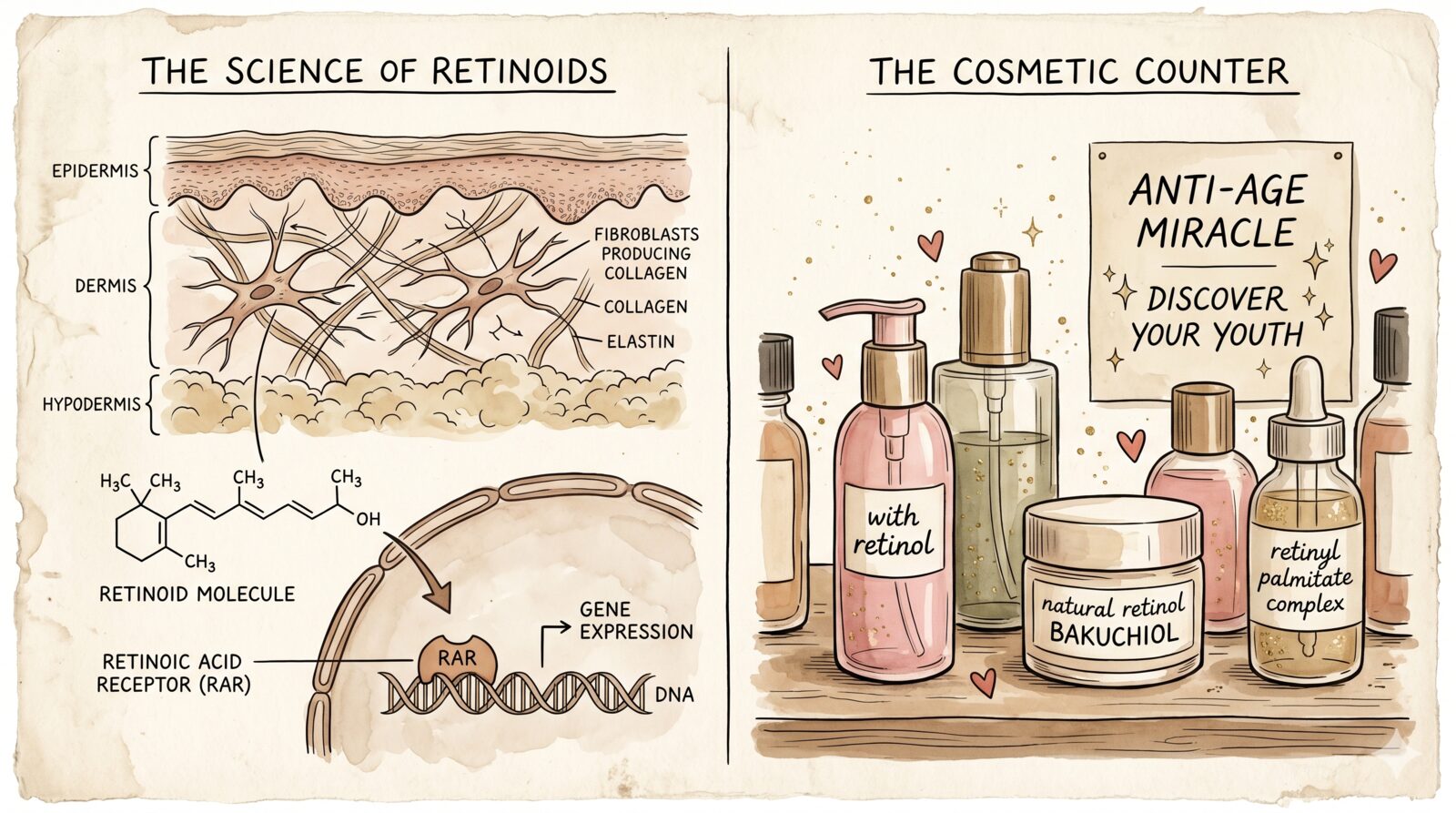
The progenitor is tretinoin (all-trans retinoic acid), a prescription drug FDA-approved since the seventies for acne and — later — for photoageing. It works by binding to the retinoid nuclear receptors (RAR), modulating gene expression in skin cells: it accelerates keratinocyte turnover, normalises keratinisation, stimulates the production of type I and III collagen, and reduces the metalloproteinases that degrade it. It is effective on acne, photoageing, dyschromia, and skin texture quality. It is not cosmetics: it is clinical dermatology.
Below tretinoin, in decreasing order of efficacy (and inverse tolerability), come its cousins:
-
Retinaldehyde (retinal): the metabolic step immediately before tretinoin. Once applied to the skin, it is converted into retinoic acid in a single enzymatic step. Documented efficacy, slightly better tolerability than tretinoin. At 0.05-0.1% it is a serious active.
-
Retinol: two enzymatic steps away from tretinoin. Lower efficacy than retinaldehyde but documented in dermatological trials. It needs higher concentrations (0.3-1%) and longer time-frames to produce detectable effects. More stable than retinaldehyde, but still sensitive to light and oxidation.
-
Retinyl palmitate, retinyl acetate: esters of retinol, further enzymatic steps away from retinoic acid. Modest or null clinical efficacy at typical cosmetic concentrations. They are often added to mass-market products so the label can read “with retinol” — it is almost always marketing.
-
Adapalene: a third-generation synthetic retinoid, light-stable, originally developed for acne. In the United States it is available over the counter; in Europe it is still by prescription. Documented efficacy on acne and skin quality, generally good tolerability.
The principle: if the label says “retinyl palmitate”, you are not using a serious retinoid. If it says “retinol” at 0.3-1% in a stabilised formulation, or “retinaldehyde” at 0.05-0.1%, you are using something the literature recognises as effective. If your skin tolerates it and you have a dermatologist following you, prescription tretinoin remains the reference standard.
4. Vitamin C: the most discussed molecule in skincare¶
Vitamin C is one of the few cosmetic actives with a scientific dossier comparable to that of retinoids. Antioxidant, modulator of collagen synthesis, brightening agent through tyrosinase inhibition. Independent randomised trials on photoageing, dyschromia, and skin quality.
The problem is that “vitamin C” in cosmetics is a cover name for at least a dozen different chemical forms, with very different efficacies.
L-ascorbic acid. The physiologically active form. The one the literature has studied most thoroughly. Effective concentration: 10-20%. Required pH: below 3.5, ideally around 2.5-3. Stability: terrible — it oxidises rapidly on contact with air, light, and heat. Serious formulations use airless packaging and co-antioxidants (vitamin E and ferulic acid stabilise ascorbic acid and amplify its effect — the C + E + Ferulic combination has been a laboratory standard since Pinnell’s 2005 studies). Good-quality L-ascorbic acid serums are the most reliable vitamin C product, but they need to be used before they turn dark yellow.
Ascorbyl glucoside, magnesium ascorbyl phosphate, sodium ascorbyl phosphate, ascorbyl tetraisopalmitate, ethyl ascorbate. More stable derivatives of L-ascorbic acid, designed to overcome its formulation problems. The question is: are they actually converted into L-ascorbic acid once in the skin? The answer is “to a variable and often small extent”. The clinical evidence is thin — some trials show modest effects, others show no significant differences from placebo. They are often more a formulation choice than an efficacy choice.
“Natural” vitamin C from plant extracts (rosehip, acerola, kakadu plum). The actual concentrations of L-ascorbic acid in these extracts are low and variable. It is more of an aromatherapy claim than a pharmacological one.
Operational principle: if you are looking for a vitamin C serum the literature recognises as effective, L-ascorbic acid at 10-20% in a stabilised formulation (with airless packaging, co-antioxidants, and appropriate pH) is the rational choice. Everything else is a formulation compromise selling the same promise.
5. Niacinamide: the quiet workhorse¶
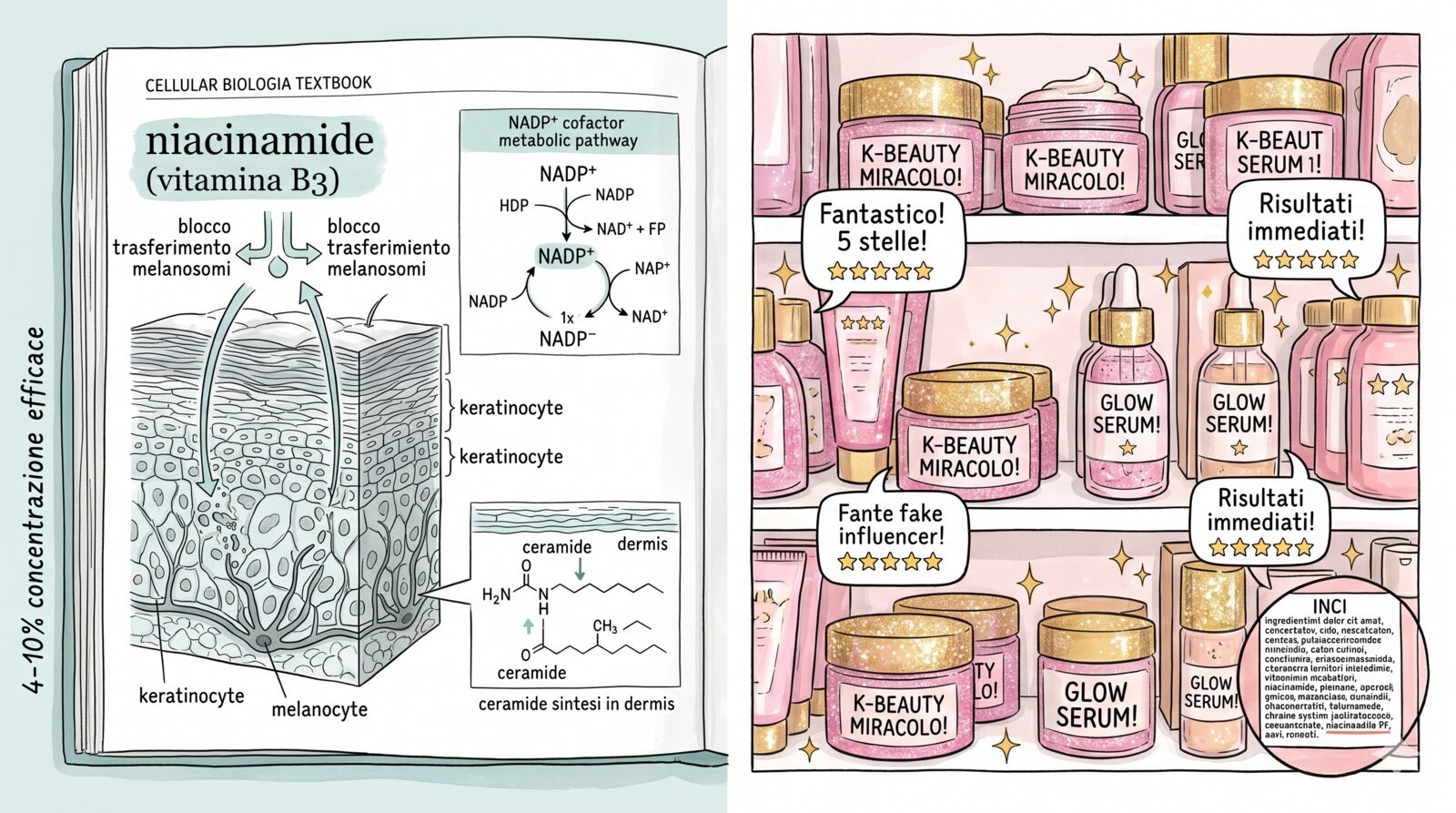
Niacinamide (vitamin B3) is probably the cosmetic active with the best efficacy-to-tolerability ratio on the market. Solid literature on skin barrier, inflammation, hyperpigmentation, sebum, and tissue quality. Stable across a wide pH range, well tolerated even by sensitive skin, synergistic with almost every other active.
Effective concentration: 4-10%. Above 10% it can cause redness without meaningful added benefit. It is one of the few actives where even mid- and low-tier products reach useful concentrations — one of the reasons niacinamide has worked its way into so many mass-market formulations, from cheap serums to pharmacy creams.
Documented effects: it reduces hyperpigmentation (by inhibiting the transfer of melanosomes from melanocytes to keratinocytes), reinforces the skin barrier (by stimulating ceramide synthesis), reduces inflammation, regulates sebum, and has a modest anti-ageing effect on fine lines. It is not a retinoid and does not replace vitamin C, but it is a serious complement to both.
When a 5-10% niacinamide product is sold at mass-market prices, it usually delivers on its promise. It is one of the rare cases where the value-for-money equation favours the buyer who is not paying premium prices.
6. Azelaic acid: the underrated one¶
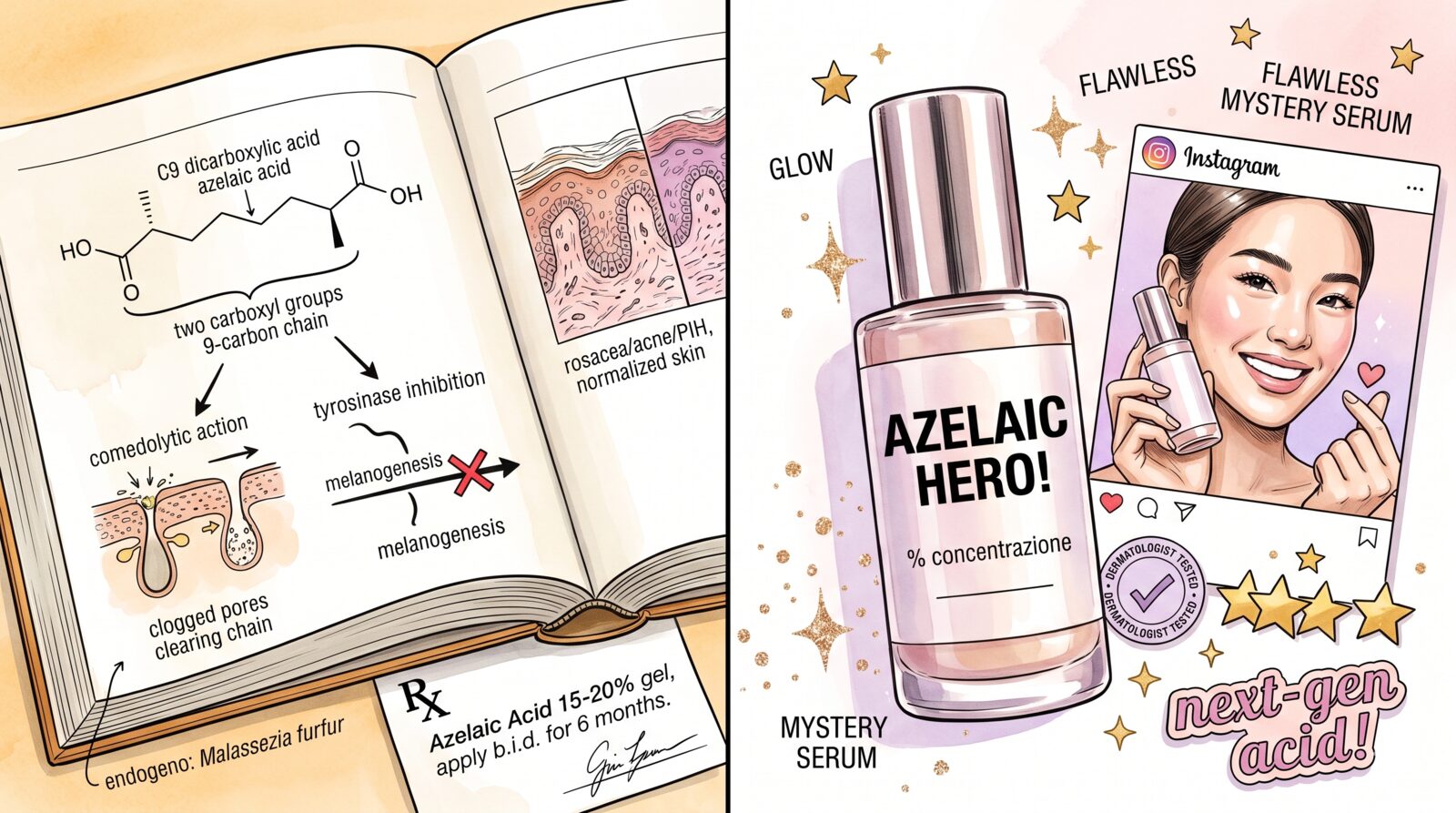
Perhaps the most underused active in everyday skincare. Azelaic acid is an endogenous molecule produced by the Malassezia yeast, with well-documented clinical evidence on acne, rosacea, and post-inflammatory hyperpigmentation. It inhibits tyrosinase (and therefore melanogenesis), has antibacterial action against C. acnes, reduces inflammation, and normalises keratinisation.
In Europe it is available as a drug at 15-20% (Skinoren, Finacea); over-the-counter cosmetic formulations at 10% also exist. Tolerability is generally good, even on sensitive skin and during pregnancy — one of the few actives compatible with that phase.
It also pairs well: with niacinamide as a duo for spots and tone, with retinoids as an anti-acne adjuvant, with vitamin C as layered work on pigmentation.
The only reason it is talked about less than vitamin C is that it is not a “sexy” molecule — it has no strong brand identity, no narrative personality. But for anyone with pigmentation problems or adult acne, it is often more useful than three trendier products combined.
7. AHA, BHA, PHA: the chemistry of exfoliants¶
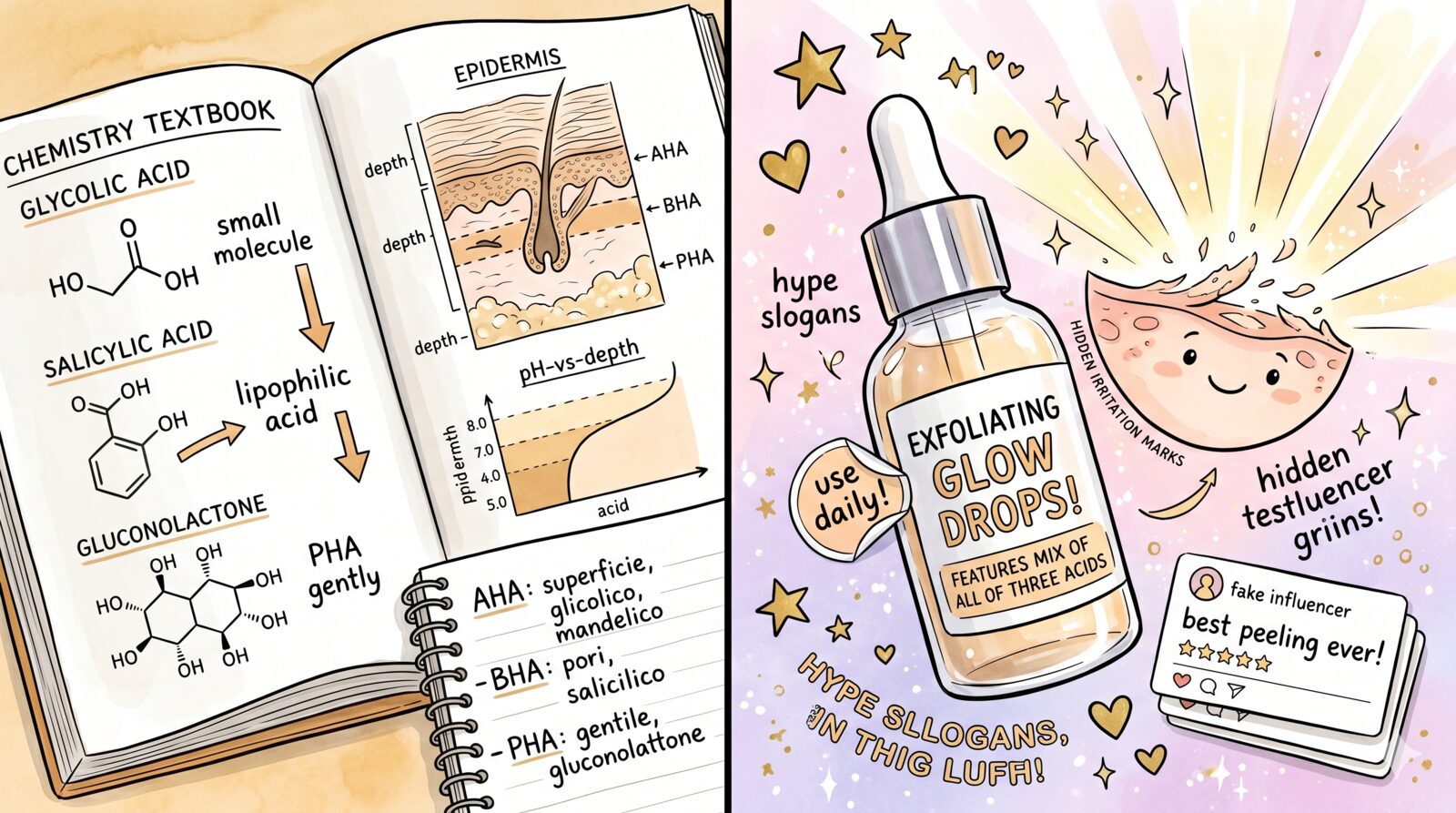
The alpha-hydroxy acids (AHA — glycolic, lactic, mandelic) and the beta-hydroxy acids (BHA — salicylic) are chemical exfoliants with solid clinical literature.
Glycolic. The most studied and the most aggressive of the AHAs. Penetrates deeply thanks to its low molecular weight. Dermatological trials document efficacy on dyschromia, photoageing, and tissue quality. Useful cosmetic concentrations: 5-10%; medical concentrations (peels): 30-70%.
Lactic. Milder than glycolic, and also moisturising. Good tolerability on sensitive skin.
Mandelic. Larger molecule, slower penetration, better tolerance on darker skin tones (lower risk of post-inflammatory hyperpigmentation).
Salicylic (BHA). Lipophilic, penetrates the sebaceous follicles. The standard for acne and oily skin. Cosmetic concentrations: 0.5-2%.
PHA (gluconolactone, lactobionic acid). Larger molecules, more superficial exfoliation, even better tolerability. A good choice for reactive skin.
The principle: good-quality chemical exfoliants work. They are a more consistent and controllable alternative to mechanical exfoliation (scrubs, granules), which often causes more micro-trauma than benefit. The typical marketing trap is convincing people that using more exfoliants, more often, in more products is better. It is not. Over-exfoliated, sensitised, barrier-damaged skin has been one of the most common dermatological problems of the last decade.
8. Sunscreen is the real anti-ageing¶
A note that belongs at the top of the article, but which we put here so as not to distract from the commercial protagonists: the single skincare measure with the greatest documented impact on photoageing is the daily use of a broad-spectrum sunscreen. It is not an opinion: it is one of the most robust findings in all of dermatology. Four-year randomised trials have shown that daily use of an SPF 15+ sunscreen significantly reduces signs of photoageing (wrinkles, laxity, texture quality) compared with as-needed use.
Every retinol serum, every vitamin C, every peel, every laser fights damage that sunscreen would have largely prevented. It is not glamorous, costs little compared with almost everything else, and the difference between a good and a bad sunscreen is much smaller than the difference between using one and not. A cosmetically pleasant formulation, applied every morning, beats a “technically superior” sunscreen you end up skipping.
Physical filters (zinc oxide, titanium dioxide) and new-generation chemical filters (Tinosorb, Mexoryl) both have well-characterised safety profiles. The “chemical sunscreens are bad” debate was largely fuelled by an FDA study on the plasma concentrations of certain filters — useful research, but one that showed no clinical harm, only measurable levels. The regulatory conclusion is to keep using them; the rational consumer’s conclusion should be the same.
9. The most persistent fluff: peptides, bakuchiol, snail mucin, plant stem cells¶
Four categories that skincare marketing of the last fifteen years has promoted with great success, and which the independent literature barely supports.
Cosmetic peptides. Short chains of amino acids with theoretical biological rationales (Matrixyl, Argireline, copper peptides). Not to be confused with the pharmaceutical peptides of medicine (insulin, GLP-1, semaglutide) that we discussed in Peptides: the chaotic frontier. Cosmetic peptides are large molecules that struggle to penetrate the stratum corneum, delivered at concentrations below any pharmacological threshold, in formulations the independent literature rarely validates. Argireline, for instance, has been sold for almost twenty years as “botox-like” — the clinical evidence is almost all industry-funded and shows modest, variable effects. The rule: paying for cosmetic peptides is paying for a biological rationale, not a proven effect.
Bakuchiol. Extract of Psoralea corylifolia, sold as “natural retinol”. The marketing argument is that it works like a retinoid without irritating. The available literature is thin: a few small trials, often industry-funded, with modest results. The biochemical premise — that it activates the same pathways as retinol — is only partially supported. It is plausible that bakuchiol has some antioxidant activity and a modest effect on skin quality, but equating it with retinoids is a marketing operation.
Snail mucin. Exploded in K-beauty and was adopted globally. Claims range from hydration to tissue regeneration. The literature is mostly Korean and industry-funded, with soft outcomes. There is some evidence on wound healing and superficial hydration, but much less than the campaigns suggest. Probably does no harm, certainly does no miracles.
Plant stem cells. Pure marketing. Plant stem cells (apple, rose, edelweiss) are plant cell cultures from which peptides and antioxidants are extracted. Saying “stem cells” triggers a mental association with regenerative medicine — an association the formulation does not support in any way. It is one of the cleanest examples of terminological prestige transfer from biomedicine to cosmetics.
To these one could add an entire long tail: exotic botanical extracts, “miracle” oils, patented thermal waters, rare ingredients of remote origin. Almost all of them, under the lens of evidence, are neutral additives — they do no harm, they do not deliver the good they promise, they mostly sell a story.
10. Skin barrier: panthenol, ceramides, and the actives that repair¶
A section that “youth” marketing tends to neglect, because selling repair is less glamorous than selling rejuvenation. Yet this is where most people — especially those who have overdone exfoliants, retinoids, or procedures — actually need to come back. The skin barrier is the ground on which everything else is played: when it works, actives deliver their effect; when it is compromised, any active becomes irritating.
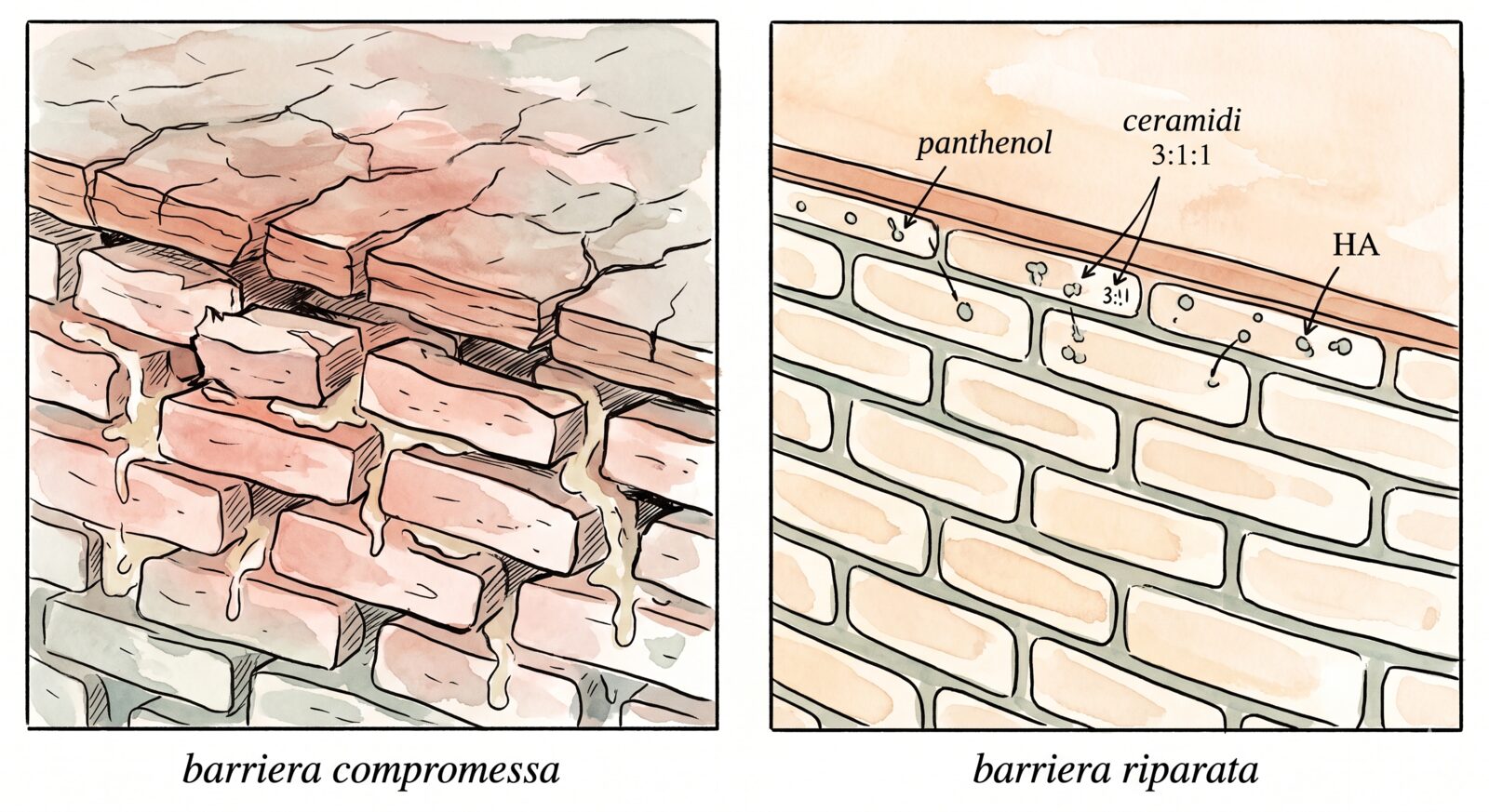
Panthenol (provitamin B5). Useful concentration 1-5%. It converts in the skin to pantothenic acid, supporting hydration, repair of the stratum corneum, and reduction of transepidermal water loss (TEWL). Particularly useful after procedures (laser, peeling, microneedling), in reactive skin, during the introduction of a new retinoid. Solid literature, well tolerated, low cost.
Ceramides, cholesterol, free fatty acids. The three lipids that make up the intercellular “cement” of the stratum corneum. The physiologically coherent ratio, supported by the work of Peter Elias and colleagues, is roughly 3:1:1 (ceramides:cholesterol:fatty acids). Serious dermo-cosmetic formulations that apply this rationale — CeraVe, La Roche-Posay Toleriane, Avène, Bioderma Atoderm — are effective, properly dosed options at affordable prices. There is no need to look for them in medical grade channels: good-quality dermo-cosmetic mass market covers this category well.
Humectants. Glycerine (safe, cheap, well-documented efficacy), topical hyaluronic acid (mostly superficial hydration), urea at low concentrations (5-10% for hydration, 10-20% for mild keratolysis on feet and elbows), panthenol itself. These are the building blocks of basic hydration. Looking for them in elaborate formulations is almost always pointless.
Reparative anti-inflammatories. Allantoin, Centella asiatica (with its triterpenes — asiaticoside, madecassoside), beta-glucan, bisabolol. A category with heterogeneous but generally positive evidence on reactive skin, post-procedural skin, mild dermatitis or rosacea. They do not replace medical treatment for significant conditions, but in sensible formulations they help the barrier recover.
A note on formulation. A good “barrier cream” combines humectants (which draw water in), occlusives (petrolatum, dimethicones, plant butters — which limit evaporation), and replenishing lipids (ceramides, cholesterol, phytosterols). A complete formulation is almost always more effective than a one-dimensional product (“hyaluronic acid serum only”, “pure oil”).
And here is where medical grade vs over-the-counter lands: the skin barrier is one of the areas where pharmacy dermo-cosmetics (CeraVe, La Roche-Posay Toleriane, Avène, Bioderma Atoderm) hold their own perfectly well against any medical grade product. Paying more for a “medical grade reparative cream” is justified only when there is a specific clinical condition (severe eczema, atopic dermatitis, aggressive post-procedural setting) followed by a dermatologist prescribing a targeted formulation.
11. Medical grade vs over-the-counter: what really changes¶
At this point, the direct question. Is medical grade worth paying for?
The answer requires unpacking what “medical grade” means. The term is not a precise regulatory label — there is no FDA stamp for “medical grade” — but it generally indicates a family of products that share certain features:
- They are typically distributed through professional channels (medical practices, dermatologists, aesthetic medicine), not mass-market ones.
- Active concentrations tend to be higher than the OTC average, and closer to the ranges studied in clinical trials.
- Formulations are often tested in dedicated clinical trials (although almost always company-sponsored).
- Packaging is often more technical (airless bottles, single-dose, dark glass) to preserve the stability of the actives.
- The price is significantly higher, both because of real costs (more expensive ingredients, technical packaging, R&D) and because of the positioning margin.
But “medical grade” is not a uniform guarantee: for some actives the technical difference is substantial and translates into clinical efficacy, for others it is marginal or non-existent. It is worth going through this active by active — because that is where the decision of where to spend and where not to is actually made.
Active by active: where it is worth spending and where it is not.
-
Retinoids (§3) — worth spending. Tretinoin (pharmacy only, on prescription) is already a drug, not a cosmetic — the comparison does not really apply here. For cosmetic retinol, serious concentrations (0.3-1%) in stabilised vehicles and airless packaging are found almost exclusively in dermo-professional ranges (SkinCeuticals, ZO Skin Health, Obagi, Medik8 with encapsulated retinaldehyde). Mass market = under-dosed or rapidly oxidised.
-
Vitamin C (§4) — worth spending, but only for L-ascorbic acid. If you are after L-ascorbic acid at 10-20% in a stabilised formulation (C+E+Ferulic, anti-oxidation packaging), medical grade is justified. If you are willing to settle for the alternative forms (ascorbyl glucoside, sodium ascorbyl phosphate, ethyl ascorbate) — less potent but also less irritating — dermo-cosmetic mass market does the job at a fraction of the price.
-
Niacinamide (§5) — not worth spending. It is the most democratic category in skincare: 5-10% niacinamide in a fifteen-euro serum works exactly as well as 5-10% in an eighty-euro one. Good-quality mass market (The Ordinary, CeraVe Niacinamide, Paula’s Choice 10%) is enough.
-
Azelaic acid (§6) — depends on the concentration. Up to 10%, dermo-cosmetic formulations (Paula’s Choice 10%, The Ordinary 10%) are valid options. For 15-20% you need a medical prescription (Skinoren, Finacea) — not “medical grade”, an actual drug.
-
AHA/BHA/PHA (§7) — almost never worth spending. The concentrations effective for home use (5-10% glycolic, 1-2% salicylic) are well covered by dermo-cosmetic mass market (Paula’s Choice, The Ordinary, La Roche-Posay Effaclar). Clinical peels at 30-70% are medical procedures, not shelf skincare.
-
Sunscreens (§8) — not worth spending. A well-formulated SPF 50 from a pharmacy (La Roche-Posay Anthelios, Avène, Bioderma Photoderm, ISDIN, Heliocare) reaches the same standards as the more expensive “medical grade” sunscreens. The difference is texture and individual tolerability, not protection.
-
The “actives” of §9 (cosmetic peptides, bakuchiol, snail mucin, plant stem cells) — never. Medical grade pricing does not make a non-working rationale any more effective. Paying more for a cosmetic peptide in an airless bottle is paying more handsomely for a fragile promise.
-
Skin barrier (§10) — almost never. Pharmacy dermo-cosmetics (CeraVe, La Roche-Posay Toleriane, Avène, Bioderma Atoderm) cover panthenol, ceramides, and reparative anti-inflammatories perfectly well at honest prices. Medical grade only makes sense in specific post-procedural protocols under medical guidance.
In short: medical grade has technical reasons to cost more only on a few specific actives — retinoids and vitamin C above all. For the rest, good-quality dermo-cosmetic mass market often reaches the same efficacy. The “medical grade” label alone is not an indicator of efficacy, and neither is the price.
Closing¶
Serious skincare, brutally summarised: a cleanser that does not damage the skin barrier, a daily broad-spectrum sunscreen, a recognised active (a retinoid in the evening, possibly a vitamin C in the morning), niacinamide or azelaic acid if needed, a moisturiser you actually like using. The rest is optional, and most of what is sold as “essential” is not.
This is also the logic on which — in the third and final part of this series — we will build an honest routine: a few right actives at the right concentrations, choosing medical grade where it really matters and mass market where it is fine as is. Without the fluff of twelve-step rituals and without the nostalgia of less is more at all costs.
Because skin, in the end, does not respond to the number of products we use. It responds to the few that actually do something, at the right doses, every day.
Essential bibliography¶
A few references, chosen for the most solid and most contested claims in this article: tretinoin as the gold standard for photoageing, topical vitamin C as L-ascorbic acid, ferulic acid as a stabiliser, niacinamide on pigmentation and signs of ageing, bakuchiol vs retinol, azelaic acid vs hydroquinone in melasma, photoprotection as the single most effective measure, the lipids of the skin barrier and panthenol as a reparative.
- Weiss JS, Ellis CN, Headington JT, Tincoff T, Hamilton TA, Voorhees JJ. Topical tretinoin improves photoaged skin. A double-blind vehicle-controlled study. JAMA. 1988;259(4):527-532. PMID: 3336176
- Pinnell SR, Yang H, Omar M, et al. Topical L-ascorbic acid: percutaneous absorption studies. Dermatol Surg. 2001;27(2):137-142. PMID: 11207686
- Lin FH, Lin JY, Gupta RD, et al. Ferulic acid stabilizes a solution of vitamins C and E and doubles its photoprotection of skin. J Invest Dermatol. 2005;125(4):826-832. PMID: 16185284
- Hakozaki T, Minwalla L, Zhuang J, et al. The effect of niacinamide on reducing cutaneous pigmentation and suppression of melanosome transfer. Br J Dermatol. 2002;147(1):20-31. PMID: 12100180
- Bissett DL, Oblong JE, Berge CA. Niacinamide: A B vitamin that improves aging facial skin appearance. Dermatol Surg. 2005;31(7 Pt 2):860-865. PMID: 16029679
- Dhaliwal S, Rybak I, Ellis SR, et al. Prospective, randomized, double-blind assessment of topical bakuchiol and retinol for facial photoageing. Br J Dermatol. 2019;180(2):289-296. PMID: 29947134
- Farshi S. Comparative study of therapeutic effects of 20% azelaic acid and hydroquinone 4% cream in the treatment of melasma. J Cosmet Dermatol. 2011;10(4):282-287. PMID: 22151936
- Feingold KR, Elias PM. Role of lipids in the formation and maintenance of the cutaneous permeability barrier. Biochim Biophys Acta. 2014;1841(3):280-294. PMID: 24262790
- Ebner F, Heller A, Rippke F, Tausch I. Topical use of dexpanthenol in skin disorders. Am J Clin Dermatol. 2002;3(6):427-433. PMID: 12113650