Abstract. BPC-157, TB-500, CJC-1295, Epithalon, MOTS-c: molecules that biohackers inject at home citing mouse preclinical data and before/after photos, without the trials we would take for granted for any other drug. Here I examine one by one what the literature actually says — the leap from mouse to human, the quality of substances on the grey market, the longevity clinics that exploit regulatory arbitrage to sell in Dubai what FDA and EMA have blocked. Follow-up to Living Forever.
On the biohacker catalogue, peptides occupy a peculiar position: more sophisticated than pharmacy supplements, more accessible than prescription drugs, wrapped in a scientific vocabulary that makes them seem like serious medicine without actually being so — not yet, perhaps never. It is a grey zone populated by real molecules, real literature, and claims that run much faster than the literature.
There are three mirror-image mistakes when discussing peptides. The first is to dismiss them as quackery: many have solid biological foundations, some have interesting preclinical literature, one or two are approaching serious clinical trials. The second is to treat them as finished drugs: none of the peptides on the grey market have the clinical documentation we would take for granted in any other therapeutic context. The third, more insidious, is to confuse mechanistic plausibility with clinical evidence. “It makes sense how it would work” is not the same thing as “we know it does good, in whom, at what doses, for how long, without which risks”. That distinction is everything.
This article tries to stand in that middle ground. To describe what they really are, where the claims come from, where the science stops and the marketing begins, and which peptides — today — have some basis to reason from, and which travel almost exclusively on anecdotes and before-and-after photos.
1. What they are, first of all¶
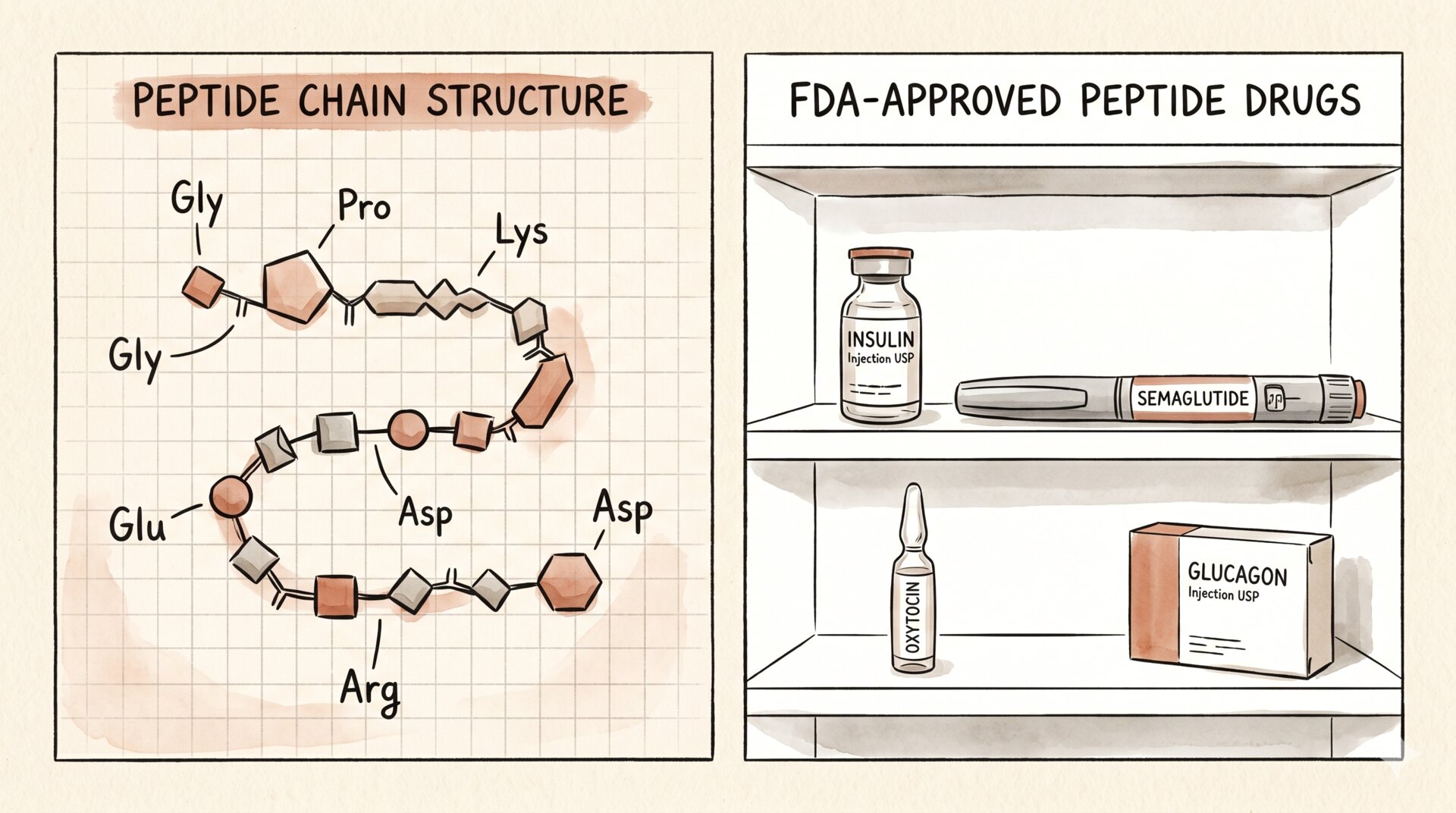
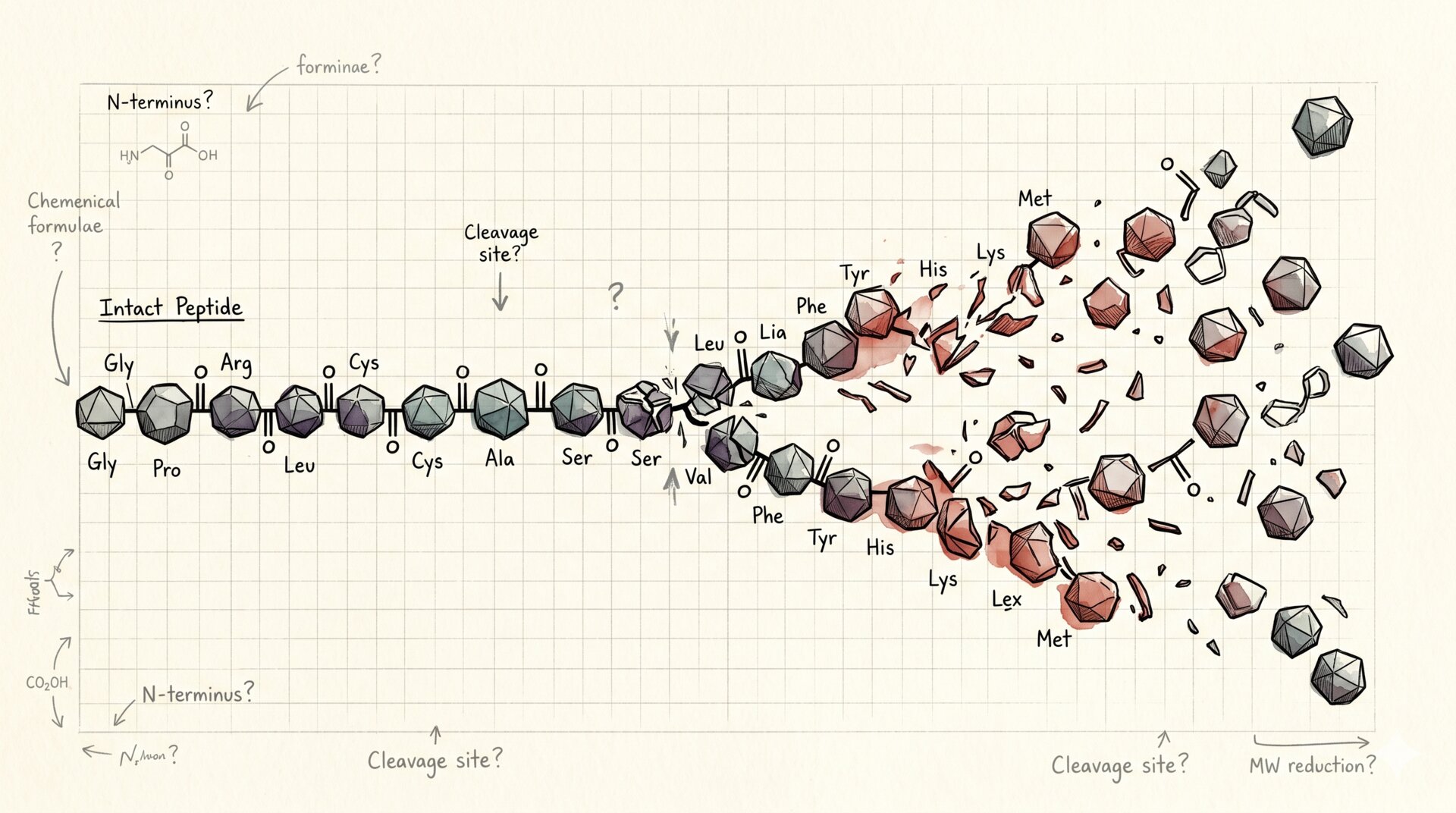
A peptide is a chain of amino acids linked by peptide bonds, shorter than a protein. Conventionally, one speaks of a peptide below roughly 50 amino acid residues; above that, you enter protein territory. It is not a homogeneous chemical class: peptides are molecules of biological communication — hormones, growth factors, neuromodulators, fragments of parent proteins — that the body has always used to make cells and tissues talk to each other.
It is not an exotic category. Insulin, oxytocin, glucagon, thyroid-stimulating hormone, GLP-1: all peptides. Peptide drugs have existed for decades, approved, studied, monitored. Medicine knows peptides well — it knows, above all, how much work it takes to develop a peptide as a drug and how much evidence is needed to use it safely.
The problem with “peptide biohacking” is not that peptides are fake. It is that many grey-market peptides have skipped the boring part — randomised trials, dose-response, pharmacokinetics, long-term monitoring — and reached the public straight from preclinical research, often translating data from mice and in vitro studies into protocols to inject at home. That leap is the real theme.
2. Where a market peptide is born¶
Every peptide in the catalogue has a real scientific biography. It is important to say this, because the sneer “it’s all a scam” is as wrong as blind enthusiasm.
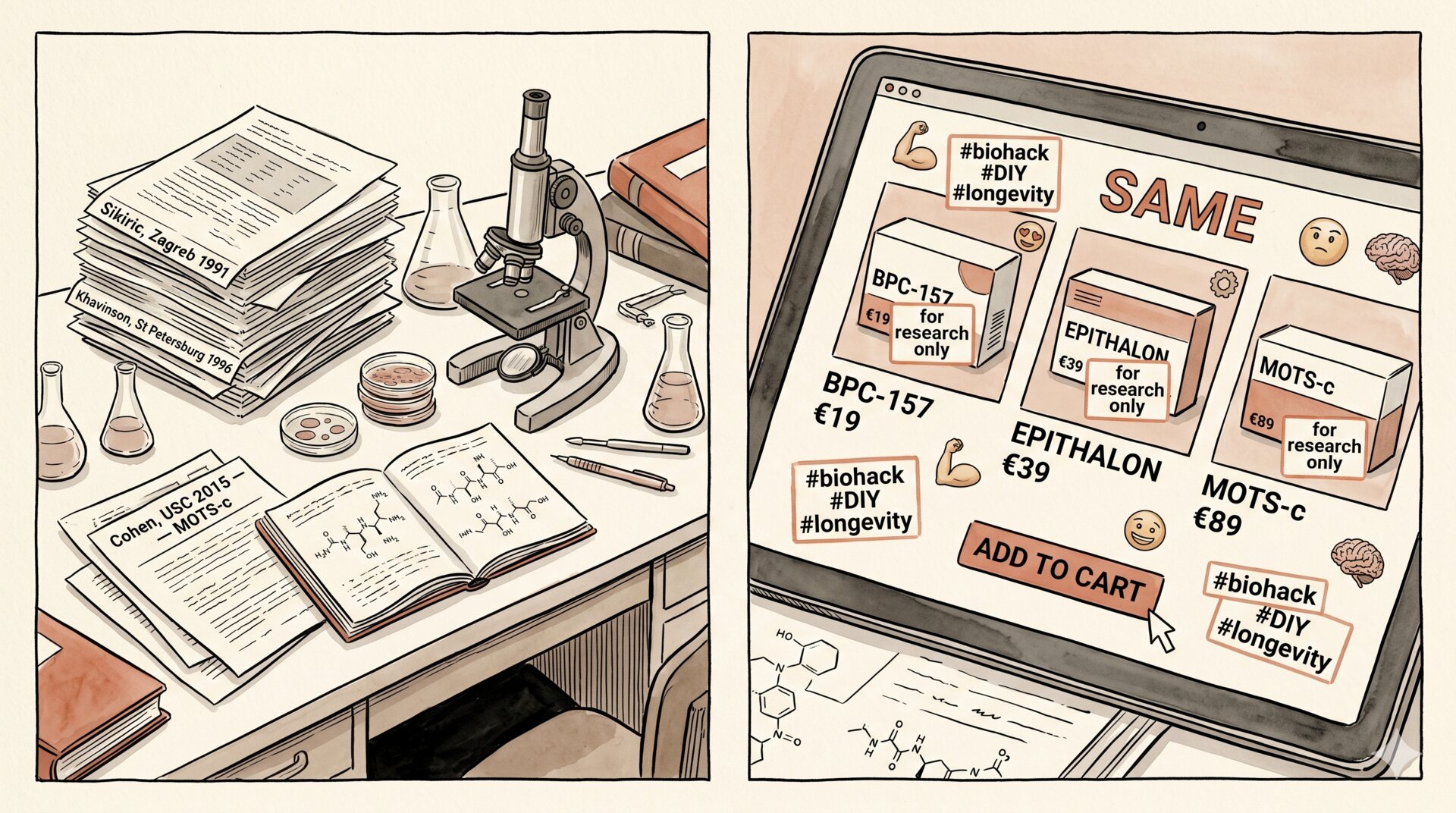
BPC-157 (Body Protection Compound 157) is a synthetic fifteen-amino-acid fragment derived from a protein identified in human gastric juice. Sikiric’s group in Zagreb has been working on it since the nineties, with an extensive scientific output in murine models: healing of tendons, ligaments, muscle lesions, gastric ulcers. The preclinical literature is real. Clinical trials in humans, documented and registered to international standards, are essentially absent.
TB-500 is the commercial name for a peptide derived from Thymosin β4, an endogenous protein involved in cell motility, tissue repair, and angiogenesis. Natural Thymosin β4 did in fact undergo clinical development — one version (RGN-259) was tested in trials for keratopathies and corneal wounds. The TB-500 circulating online, however, is often a smaller fragment, produced in non-pharmaceutical chemical labs, with variable quality and identity. The link between “TB-500 bought online” and “Thymosin β4 with clinical data” is often weaker than the name suggests.
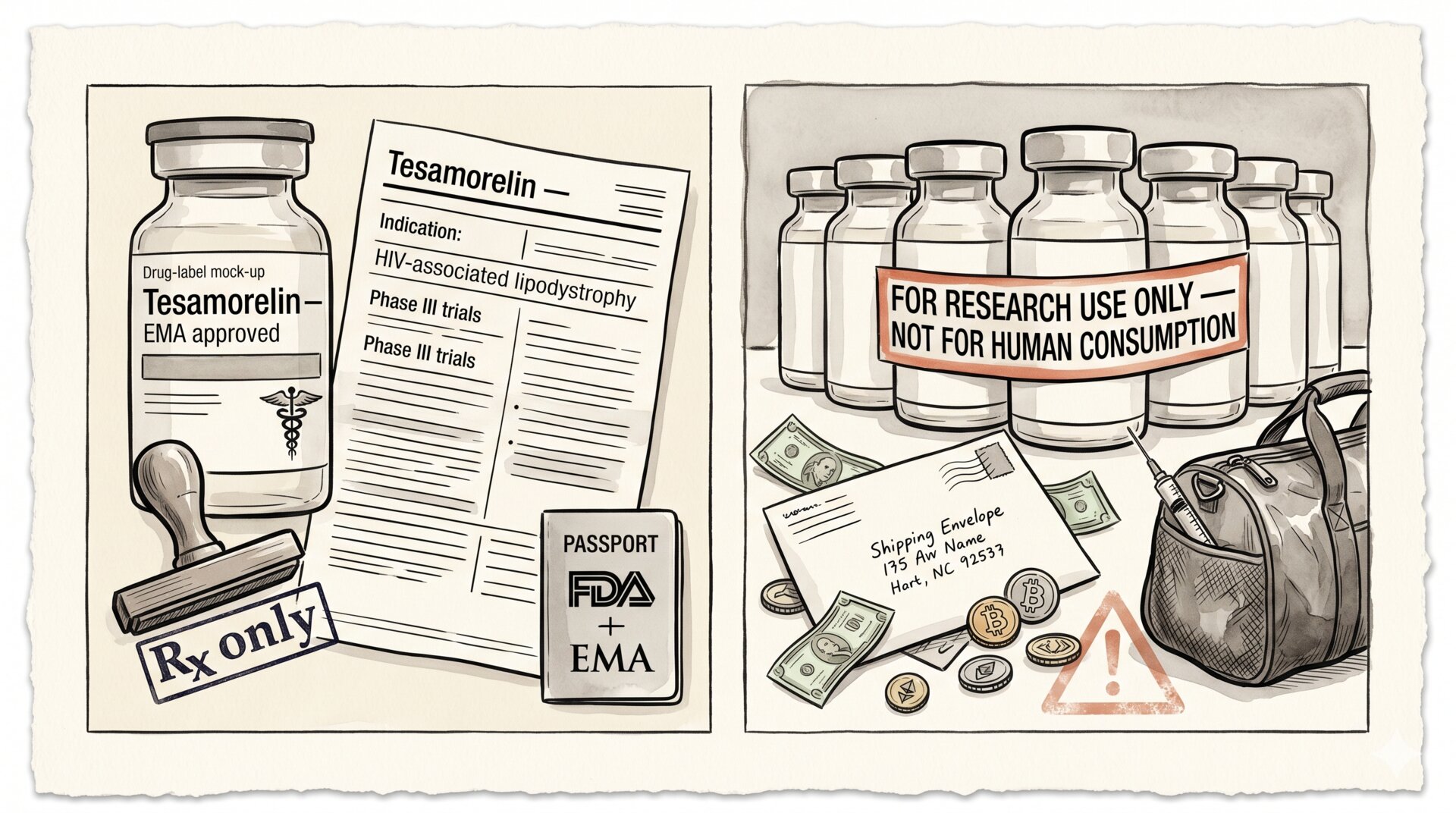
GH secretagogues — CJC-1295, Ipamorelin, Sermorelin, Tesamorelin, Hexarelin — are molecules that stimulate the endogenous release of growth hormone from the pituitary, mimicking or amplifying natural signals (GHRH, ghrelin). Sermorelin was for a long time an approved drug; Tesamorelin still is, for HIV-associated lipodystrophy. The others live almost exclusively in the compounding market and the “research only” catalogue. The pharmacological rationale is real; the distance between “stimulating endogenous GH” and “obtaining clinical benefits without risks” is, as we shall see, greater than is usually told.
Epithalon (or Epitalon) is a tetrapeptide developed by Vladimir Khavinson at the Institute of Bioregulation and Gerontology in Saint Petersburg, with claims of telomerase activation and modulation of pineal function. Much of the literature is in Russian, with methodological standards that do not always overlap with those required by Western journals. The independence of replications is limited. The rationale directly evokes the myth of telomerase as the fountain of youth — a myth which, as already seen, is more complicated than it is sold.
MOTS-c is a mitochondrial peptide discovered by Pinchas Cohen’s group at USC. It is the most interesting case scientifically: the preclinical literature on metabolism, insulin sensitivity, and the response to exercise is solid and replicated, and the first human clinical studies are underway. It is also the peptide you will hear least about online, because it does not yet have a protocol that is easy to sell.
The GLP-1s — semaglutide, tirzepatide, liraglutide — are peptides too. They deserve mention precisely by contrast: they were developed following all the rules — randomised clinical trials on tens of thousands of people, multi-year follow-ups, regulatory monitoring, FDA/EMA approval. The result is that we know — with a rare degree of detail — in whom they work, at what doses, with what side effects, for which indications. It is the perfect counter-example: it is not that peptides “cannot be serious drugs”. It is that the ones taken seriously become so.
3. The leap from mouse to human¶
There is a phrase that recurs in the preclinical papers of almost every peptide in the catalogue: “these findings warrant further investigation in human subjects”. That phrase is not a rhetorical formality. It is the acknowledgement, by the authors themselves, that a result in an animal model is an interesting hypothesis, not a transferable conclusion.
The reason is banal and implacable. Rats and mice share much cellular physiology with humans — enough to use them as models, not enough to let us skip verification in humans. Pharmacokinetics, metabolism, immunological profile, tissue composition, oncological trajectories: everything changes, often non-linearly, when moving from the murine model to the human being. The history of pharmacology is full of molecules that looked miraculous in mice and produced no effect in humans — or worse, caused harm. It is one of the reasons clinical trials exist. It is not bureaucracy. It is the way we know whether something works.
The list is long, but a few cases pin down the principle better than any abstract argument.
Fialuridine (FIAU), an antiviral for hepatitis B, had passed rodent and non-human primate studies without warning signals. In the National Institutes of Health Phase II trial in 1993, it proved to be cumulatively and delayed mitochondrially toxic: five patients out of fifteen died of hepatic failure and lactic acidosis, others survived only thanks to liver transplantation (McKenzie et al., New England Journal of Medicine, 1995). The mechanism — slow accumulation in hepatic mitochondria — was simply invisible to the time windows of animal models. The mouse does not live long enough to show it to you.
TGN1412, a superagonist anti-CD28 monoclonal antibody, had been tolerated without significant adverse events by mice and cynomolgus monkeys at doses up to five hundred times greater than the one planned for humans. At first administration in six healthy volunteers, in 2006 at Northwick Park, it triggered a multi-organ cytokine storm in all six within an hour, with multi-system failure and permanent consequences for some (Suntharalingam et al., New England Journal of Medicine, 2006). The CD28 receptor behaved qualitatively differently in human T lymphocytes than in those of the animal model. No dose escalation would have saved that trial: the biology of immunity was not scalable across species.
Torcetrapib, a CETP inhibitor developed by Pfizer, raised HDL cholesterol by almost 60% in animal models and early human data. Every biomarker said “cardiology revolution”. The ILLUMINATE trial, halted early in 2006, showed a 58% increase in mortality in the torcetrapib arm compared to control (Barter et al., New England Journal of Medicine, 2007). The biomarker moved in the “right” direction. The clinical outcome moved in the opposite direction. A non-trivial distinction — and a principle that holds every time you measure a proxy hoping it represents the thing.
And there is the case most pertinent to our discussion, because it concerns exactly the territory of longevity: resveratrol. In 2006 David Sinclair’s group published in Nature that resveratrol extended the life of obese mice and mimicked many effects of caloric restriction (Baur et al., Nature, 2006). The molecule became a symbol of pharmacological anti-ageing, with tens of thousands of press pages and an entire supplement market built around it. After almost twenty years of human clinical trials, the results are, to use the technical formula, disappointing: modest metabolic effects, often inconsistent across studies, no translation into longevity outcomes (review in Berman et al., Clinical Nutrition, 2017). The mouse had been optimised. The human had not.
These are not rare or anomalous cases. They are how pharmacology works. And they are the reason human clinical trials — expensive, slow, imperfect — are not bureaucracy but epistemology.
The gap is not only efficacy: it is safety over time. A peptide injected for a few weeks into a lab rat under controlled conditions tells us almost nothing about what happens to a human being who takes it for years, perhaps in combination with other substances, perhaps during a window of life in which a silently pre-neoplastic cell is deciding what to become. Chronic effects over decades are invisible to animal studies — mice do not live long enough — and invisible to short clinical trials.
Anyone selling a peptide protocol “based on scientific data” is, in most cases, making a huge extrapolation. Not necessarily in bad faith. But extrapolation is extrapolation, and whoever buys it — with their own body — should at least know it.
4. Quality, sterility, identity¶
There is a dimension of the problem that passes completely under the radar of public discussion about peptides, and that is perhaps the most concrete: what is really in the vial?
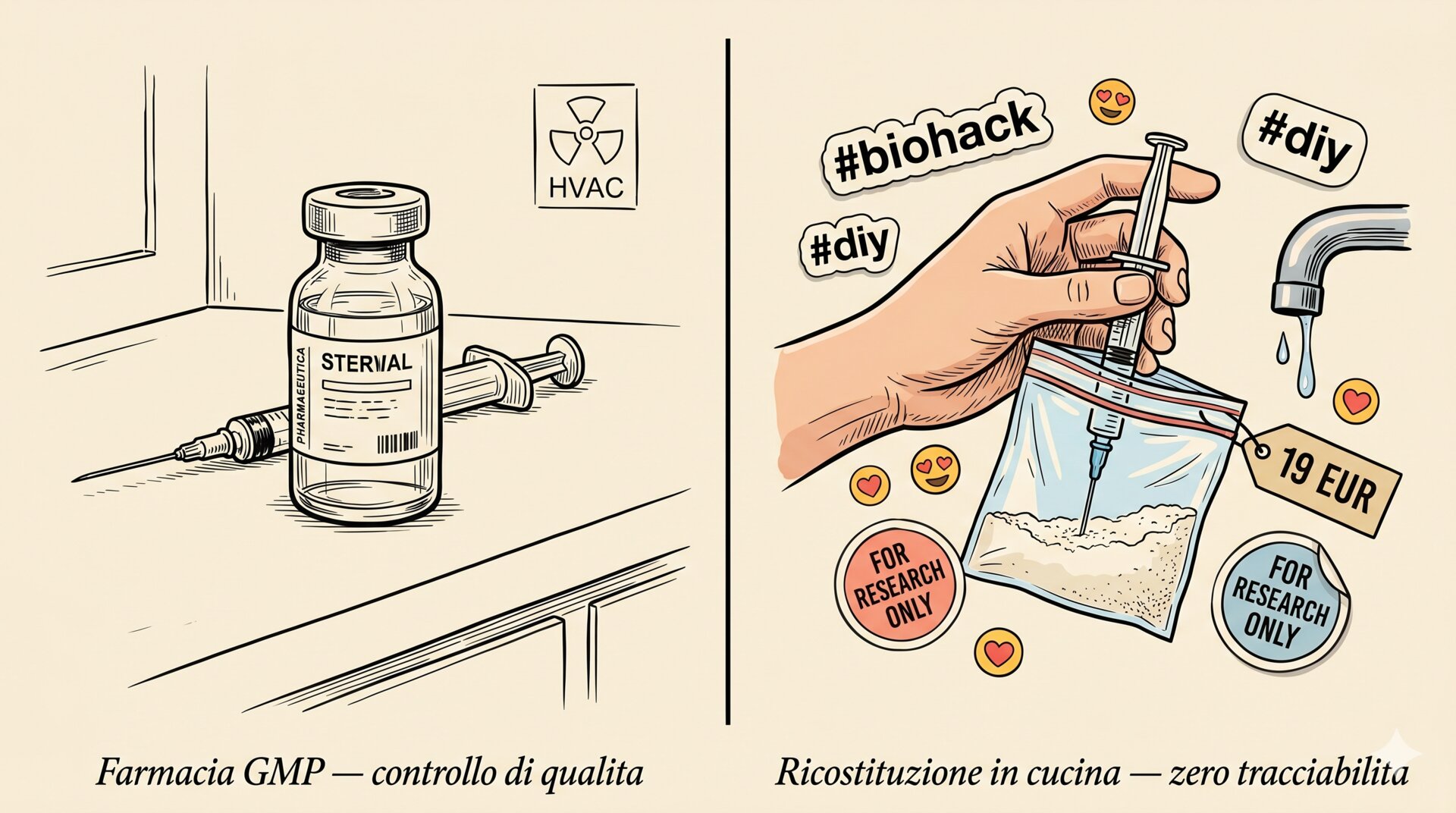
Grey-market peptides are largely produced by chemical laboratories — often in China, sometimes in Eastern Europe — which sell them with the label “for research purposes only, not for human consumption”. That phrase is not a decorative legal precaution: it is an operational disclaimer indicating that the material was not manufactured under pharmaceutical Good Manufacturing Practice. There is no sterility control, no precise quantification of the active ingredient, no characterisation of impurities, no batch traceability at the level required for a human drug.
Independent analytical tests on samples purchased from online suppliers have shown, repeatedly, impressive variability. Same name, different suppliers: different concentrations, different purity, different contaminants. Sometimes the declared peptide is present at a fraction of what the label indicates. Sometimes it is present together with unidentified peptide fragments. Sometimes it is simply not what the label says.
Then there is sterility. Peptides are sold as lyophilised powder, to be reconstituted in bacteriostatic water or sterile saline. Reconstitution done at home, storage done at home, injection done at home. Every step is an occasion to introduce microbial contamination. Abscesses, cellulitis, systemic infections from home peptide injections are documented in the emergency medical literature. They are not rare events in absolute terms — they are underreported because whoever shows up in the emergency department with a glute abscess does not always declare what they injected into it.
And once in circulation, peptides that are not peptides foreseen by the body can trigger immune responses. Immunogenicity is a known theme in peptide pharmacology: even approved therapeutic peptides have monitored immunogenic profiles. For grey-market peptides, this characterisation simply does not exist. Neutralising antibodies that switch off the peptide itself, acute allergic reactions, cross-reactivity phenomena with endogenous peptides: all possible, all under the radar, all to be discovered at the moment they happen.
5. The risk you don’t see: IGF-1, GH, and cell proliferation¶
The chapter on GH secretagogues deserves a pause. Because this is where the discussion of peptides directly intersects the one on longevity.
CJC-1295, Ipamorelin, Sermorelin, Hexarelin work — or at least, are supposed to work — by increasing the endogenous release of growth hormone from the pituitary. GH in turn stimulates hepatic production of IGF-1, which is the principal mediator of many effects attributed to GH: muscle protein synthesis, lipolysis, tissue regeneration, some effects on body composition.
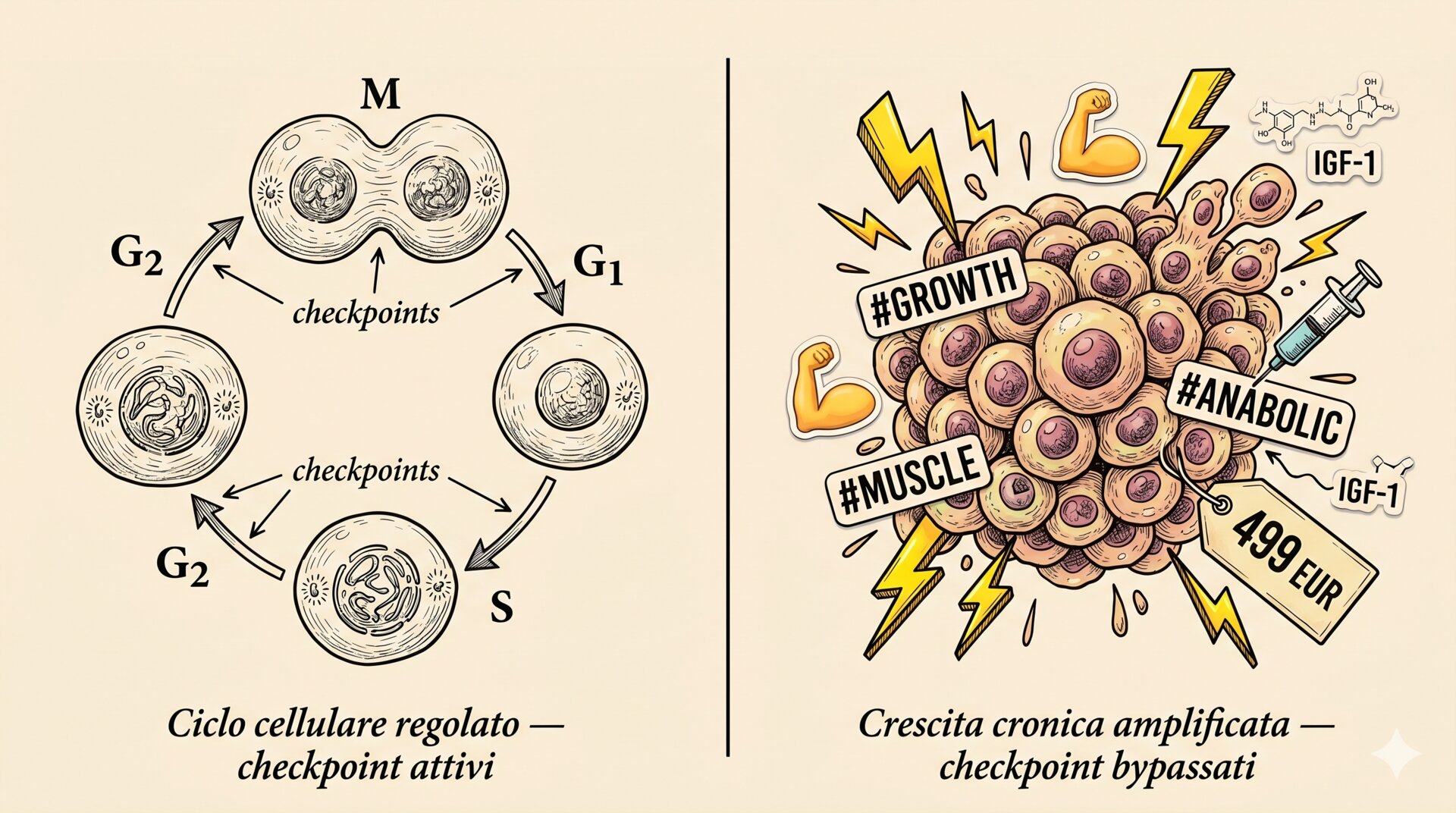
The problem is that GH and IGF-1 are not generic signals of youth. They are signals of cell proliferation. Their main biological role is to tell cells to divide, grow, survive. In a young, growing body, the signal is needed. In an adult body, with somatic cells that accumulate mutations with age — and that in most cases suppress the growth of anomalous clones through checkpoints and senescence — chronically amplifying that signal means amplifying it also for the cells that should not be growing.
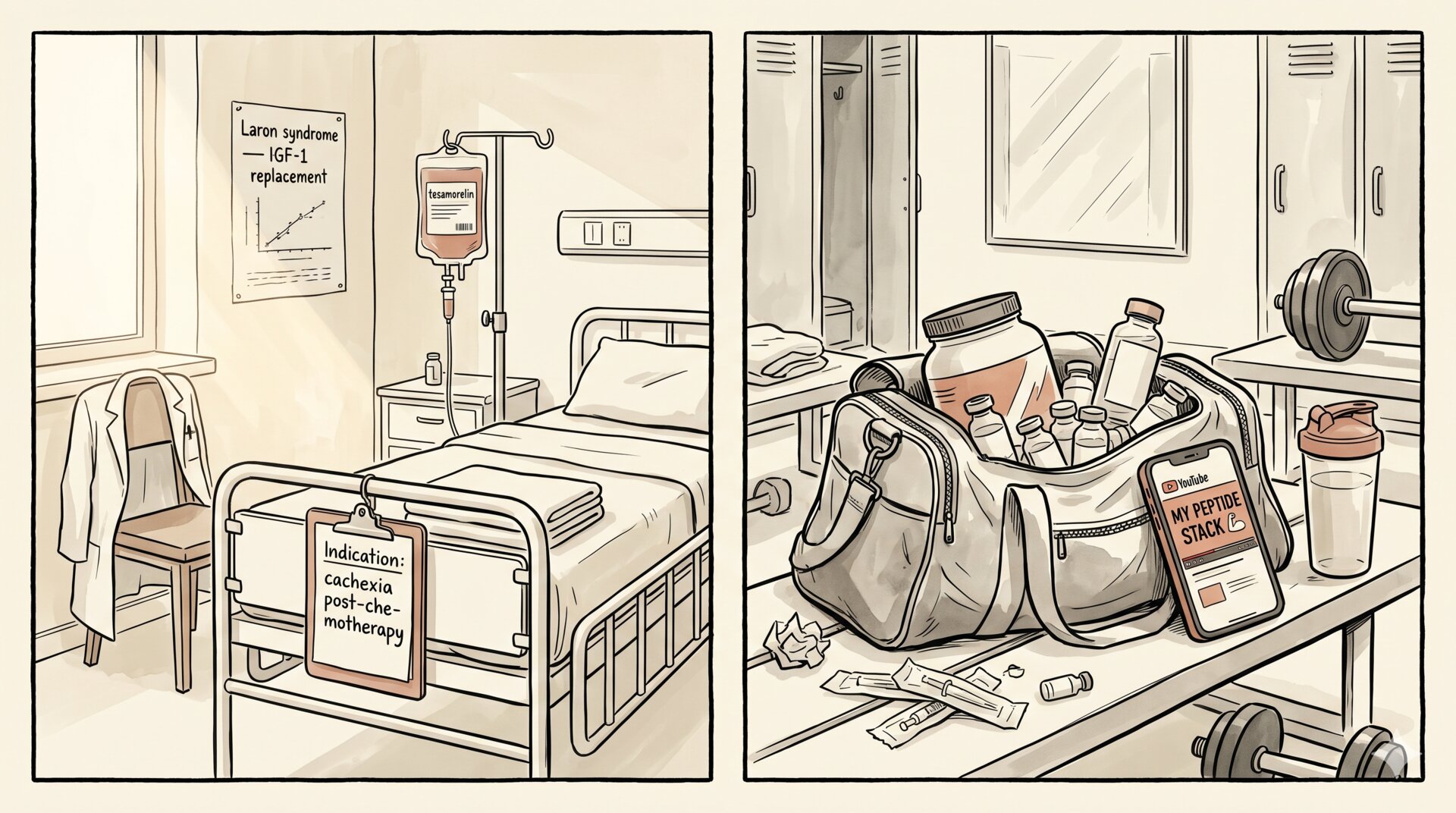
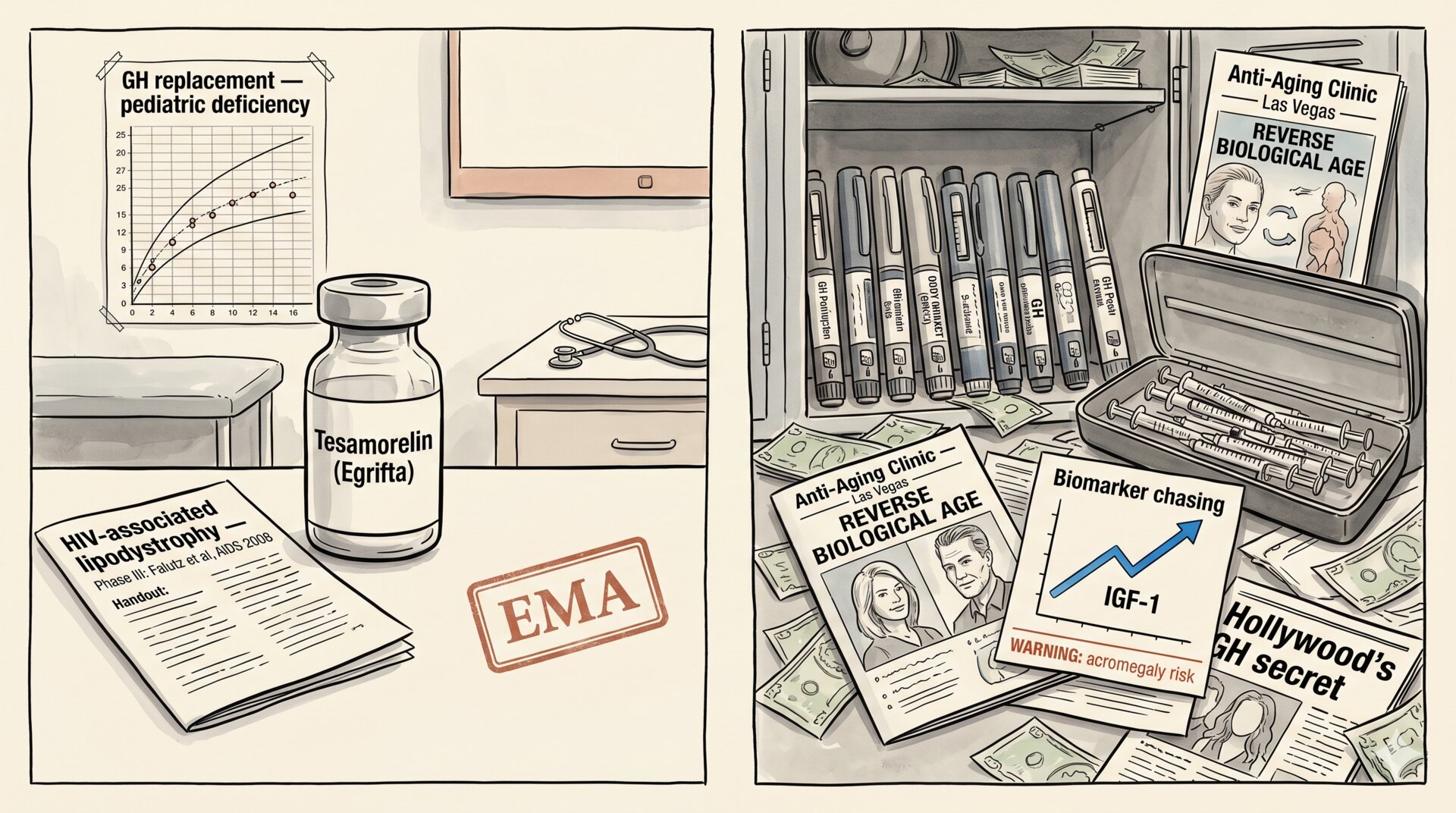
The evidence converges from several directions. Acromegaly, a condition in which the pituitary produces excess GH endogenously, is associated with cancer mortality two to three times higher than the general population, with documented excess in colon, thyroid, breast, and prostate. Caloric restriction, one of the few interventions with solid evidence of increased lifespan in many animal models, reduces precisely the levels of IGF-1. People with Laron syndrome — congenital resistance to GH — have very low IGF-1 and, at the same time, reduced incidence of tumours and diabetes.
It is not a detail. It is the pattern: the GH/IGF-1 signal is a “growth” signal, and growth everywhere, chronically, is a definition of oncogenic risk. Giving, chronically, peptides that increase that signal — even at modest doses, for years — without human data on long-term cumulative risk is exactly the type of experiment that clinical pharmacology was built to avoid.
Let us add that monitoring, once again, is a partial illusion. Serum IGF-1 is measured and the dose is decided. But the GH/IGF-1 signal acts locally on tissues, and the circulating level does not always accurately reflect chronic tissue exposure. A pre-neoplastic cell in prostatic or intestinal tissue responds to the signal it receives, not to the value you read on the lab report.
6. Epithalon, telomeres, and easy myths¶
A peptide that deserves a specific word is Epithalon, because it concentrates on itself one of the most persistent mythologies of longevity: the idea that lengthening telomeres lengthens life.
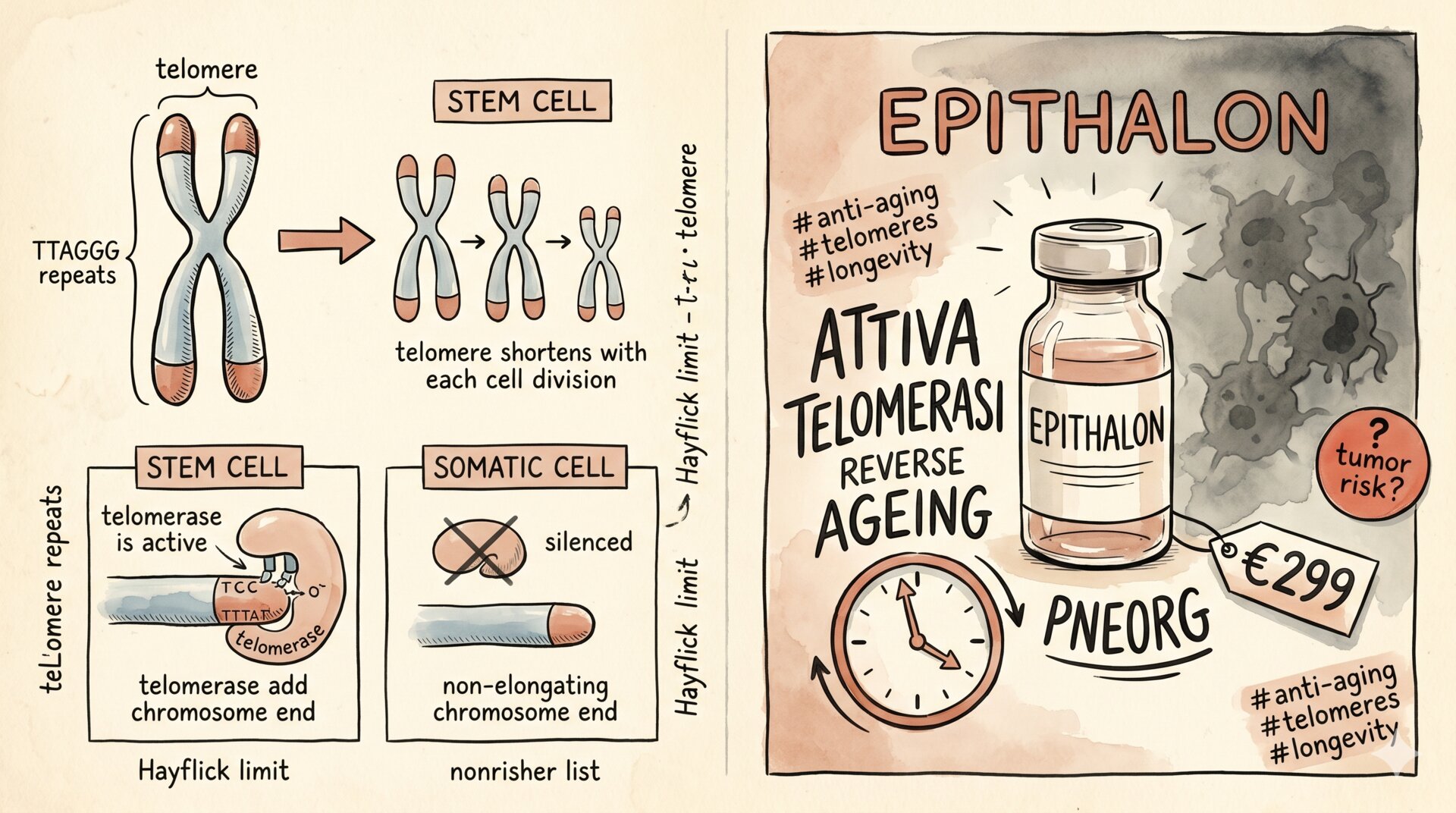
Telomeres are the repetitive sequences at the ends of chromosomes. They shorten with every cell division. When they reach a critical length, the cell enters senescence. Telomerase is the enzyme that lengthens them; it is active in germ cells and stem cells, silenced in most somatic cells. The intuition — “activate telomerase to stop cellular ageing” — is elegant. The biology is less elegant.
First problem: many tumours already reactivate telomerase aberrantly. It is one of the mechanisms by which tumour cells bypass the division limit. Activating telomerase systemically means removing one of the evolutionary mechanisms of anti-tumour protection. Murine models in which telomerase expression is forced show, in some contexts, increased tumour incidence. Not always, not in every context — but enough to require much greater caution than circulates online.
Second problem: the evidence that Epithalon really activates telomerase in humans, significantly and durably, is weak and methodologically problematic. Much of the data comes from Khavinson’s original group, with scarce independent replication. Some studies show correlations with markers of ageing; the difference between correlation and causation, and between real effect and measurement artefact, is the same we encountered discussing epigenetic clocks. The proxy is not the thing.
Third problem: even granting that it works as declared, we do not know whether the effect on telomeres in human somatic cells — if present — produces clinical benefits, or produces them, potentially, at the cost of increased oncogenic risk in the long term. We do not know because no one has studied it with the rigour it would take to know.
Epithalon is a textbook case of the peptide trap: interesting biological hypothesis, suggestive preclinical data, zero robust clinical trials, but marketing built as though the reckoning had already been done.
7. MOTS-c, or how to do it right¶
It is worth spending a section on MOTS-c, because it represents exactly the counter-example of how an emerging peptide can be seriously addressed.
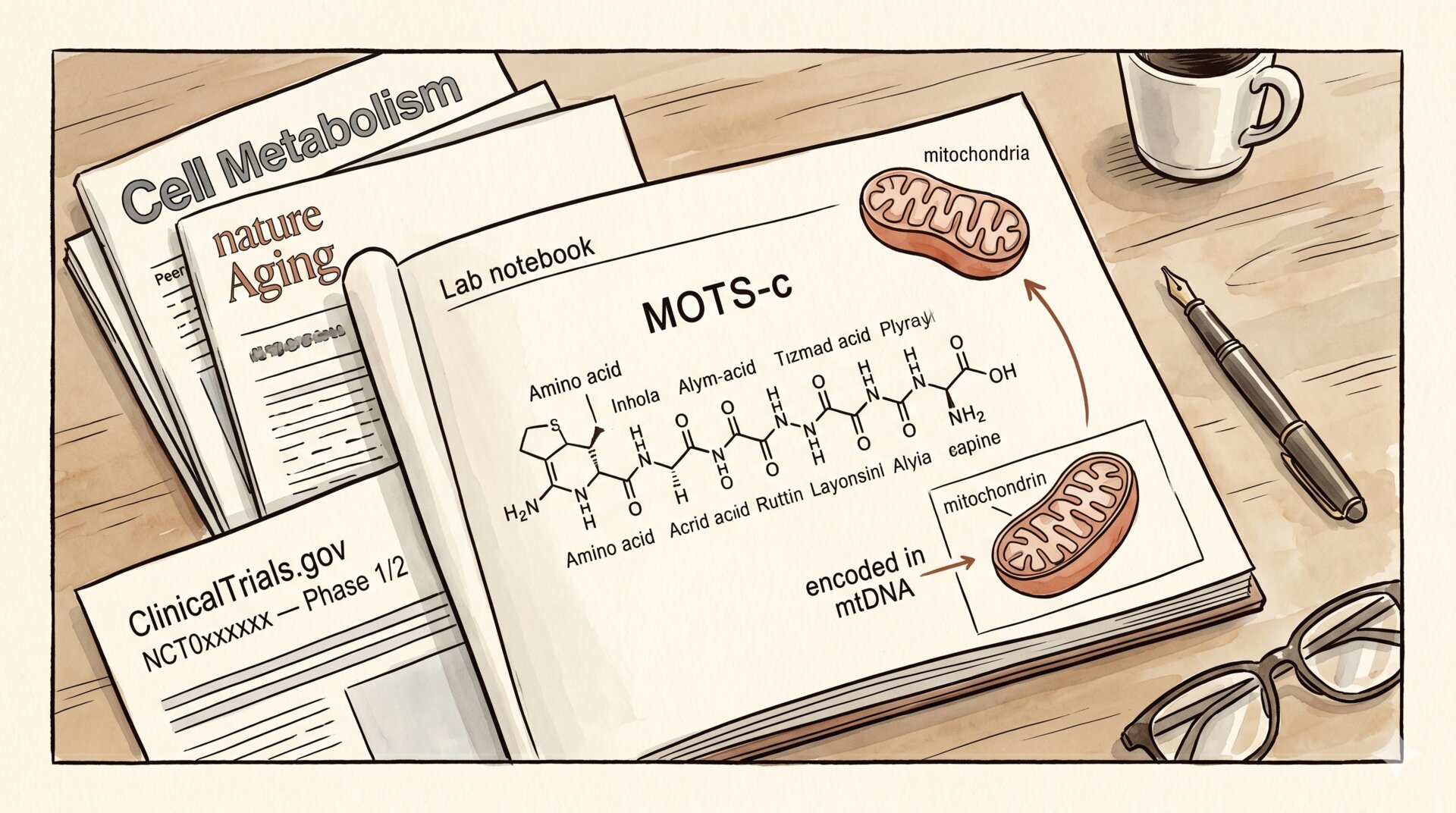
Discovered in 2015 by Pinchas Cohen’s lab at USC, MOTS-c is a 16-amino-acid peptide encoded in mitochondrial DNA — a discovery that opened a line of research into peptide communication of mitochondrial origin. The preclinical effects are consistent and replicated: improved insulin sensitivity, modulation of glucose metabolism, protection against hepatic steatosis, amplification of the metabolic response to exercise in murine models.
The literature has grown in orderly fashion: from basic biology, to validation in multiple models, to the first mechanistic studies, up to the first human clinical trials, which are currently underway at multiple centres. Preliminary human data are interesting, but still interim data — not conclusions. The regulatory pathway is active, safety monitoring is under way, pharmacokinetic characterisation is emerging.
MOTS-c is — today — the peptide with the cleanest scientific trajectory among those cited in the longevity discussion. It is also, not coincidentally, the one around which you find the least noisy marketing. Because those studying it seriously do not yet have conclusions to sell, and those who would like to sell it do not yet have enough concrete claims on which to build a catalogue.
If MOTS-c lives up to the promises of the preclinical data in the coming years, it will become a therapeutic molecule approved via the long road. If it does not, we will know with a degree of certainty that the other peptides in the catalogue will never allow us to reach. In either case: the method is the right one. It is the reason MOTS-c is science, and much of the rest of the catalogue is market with scientific vocabulary.
8. Regulation, what actually happens¶
A note on the regulatory framework, because here the ambiguity is often used as a commercial advantage.
The FDA has progressively tightened its position on grey-market peptides. In November 2023 it removed BPC-157 from the list of substances usable in compounding by 503A pharmacies, flagging safety concerns and insufficient pharmacological characterisation. Other peptides — CJC-1295, GHRP-6, Ipamorelin in some formulations — have been the subject of similar warnings or of revisions to their inclusion in authorised compounding lists. It is not a uniform ban, and it is evolving, but the direction is clear: what is easily found online is not an authorised drug in any Western healthcare system.
WADA, the World Anti-Doping Agency, includes practically all the relevant peptides in the catalogue — BPC-157, TB-500, CJC-1295, Ipamorelin, the other GH secretagogues — on the lists of prohibited substances. This is not a moral judgement: it is an acknowledgement that these molecules have the potential to alter performance and recovery, and that there is no scientific consensus on their long-term safety profile.
In Italy and in Europe more broadly, most of these peptides are not authorised as medicinal products. Purchase “for research purposes only” is not a constraint binding the end user, but it does not signify authorisation for human use. It simply means that no one has verified what happens to a human being who uses them.
9. Why it seems to work even when it doesn’t¶
An aspect that rarely appears in online testimonials is the collection of mechanisms that produce a perception of efficacy even in the absence of any real effect of the peptide.
Natural healing on physiological timeframes. A strained tendon heals in 6-12 weeks. A ligament in 4-6 months. A gastric ulcer in a few weeks. If you start BPC-157 in that period and heal on the timescale you would have followed anyway, causal attribution to the peptide is almost inevitable — and almost always impossible to verify without a control group.
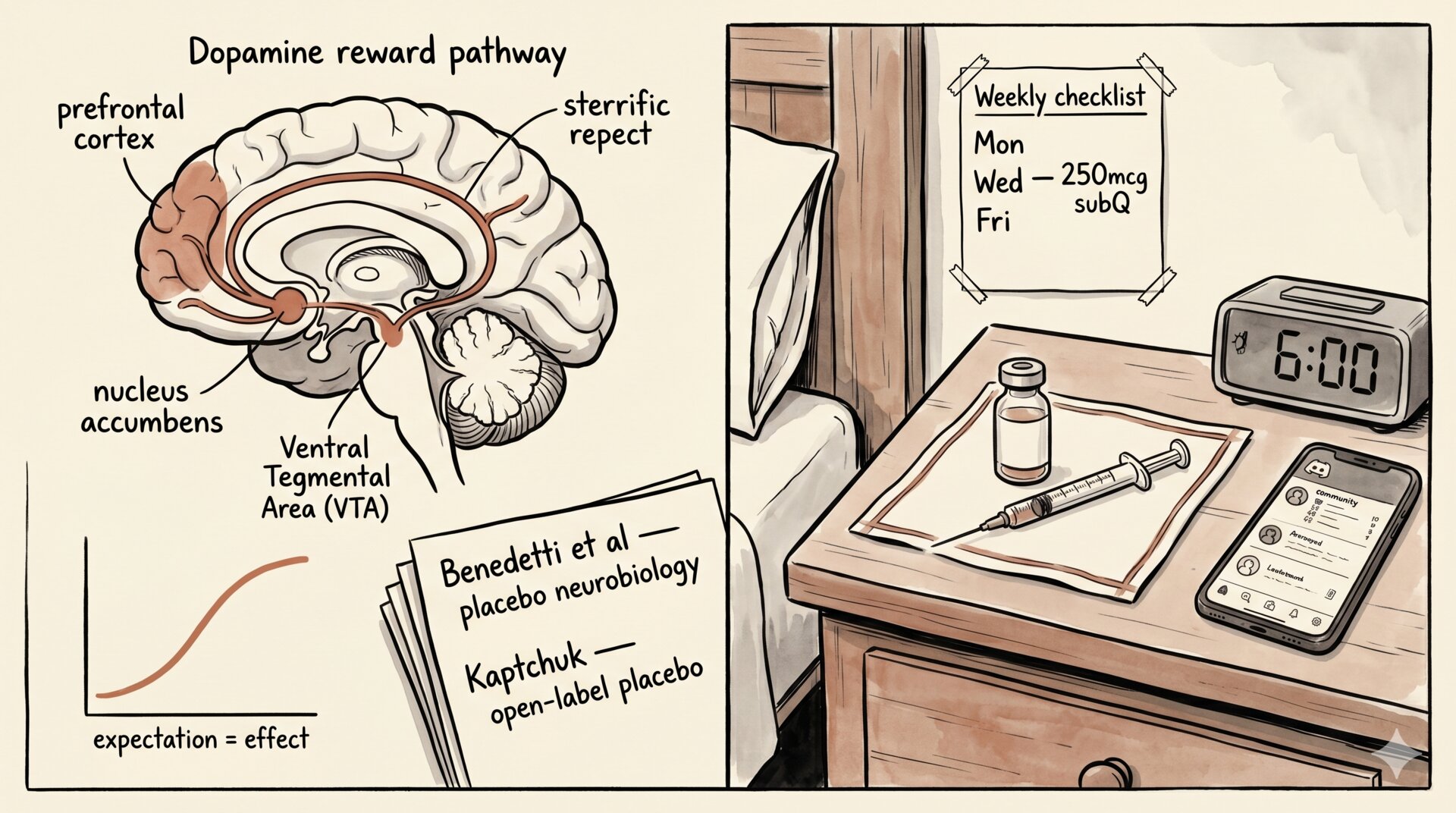
Placebo effect and active placebo. Placebo produces real, measurable effects, especially on subjective symptoms such as pain, energy, mood, libido. Injection increases the placebo effect relative to oral administration. Expensive, ritualised injection, part of an identity, increases it further.
Confirmation bias. Whoever invests time, money, and identity in a protocol has systematic biases towards reporting improvements and under-reporting absence of effect. It is human, no one’s fault, but it is statistically relevant.
Confounding with other interventions. Whoever starts a peptide cycle rarely does so in isolation. Often they pair the peptide with a phase of greater attention to sleep, nutrition, training. Those changes have real effects. The peptide collects credit for interventions that worked anyway.
Regression to the mean. You start a peptide when you are worst off — tendon pain, chronic fatigue, symptoms. Statistically, after a worsening the probability of improvement is high independently of the intervention. The peptide coincides temporally with the improvement that would have come anyway.
None of these mechanisms excludes that the peptide may have a real effect. But it means that an individual testimony — “it worked for me” — is not sufficient evidence to infer causality. It is an observation. Observations serve to generate hypotheses, not to validate them.
10. Who really benefits — and how¶
The picture, as drawn, seems to leave little room for the peptide as a useful tool. This is not so. The space is there, and it is important to delimit it honestly.
Monitored medical contexts. Sermorelin and Tesamorelin have been used in specific indications with clinical monitoring. GLP-1 agonists such as semaglutide have transformed the treatment of type 2 diabetes and severe obesity. In these cases we have informed prescription, dose adjusted to the individual, safety monitoring, and a calculable risk-benefit ratio. It is medicine. It works.
Registered clinical trials. Whoever wants to expose themselves to a still-experimental peptide, doing so sensibly, has one option: seek out a formal clinical study. With monitoring, informed consent, traceability, and the certainty that at least someone is collecting the data to understand whether it works and at what price. It is the difference between participating in the construction of knowledge and self-administering an uncharacterised molecule in the dark.
Specific rehabilitation contexts. In some specialised centres — elite sports medicine, post-surgical rehabilitation, regenerative medicine with medical supervision — some peptides are used off-label with informed consent and structured follow-up. The picture is not the online Wild West: it is a clinical context that accepts uncertainty by declaring it.
The rest — peptide bought online, reconstituted in the kitchen, injected in the gym, dosed on the basis of a YouTube video — is not a longevity protocol. It is a self-experiment without an ethics committee, without monitoring, without data collection, with a time horizon that does not cover the window in which harms might manifest. Whoever does it has the right to do so. Knowing what they are doing is another question.
11. Legitimate clinical use of GH secretagogues¶
Having said all the rest, it is important to close the circle on the point where GH and its secretagogues really become medicine. Because they exist — and are neglected by online discourse precisely because they are not very spectacular.
Adult GH deficiency. When the pituitary does not produce enough growth hormone — due to an adenoma, surgical removal, radiotherapy, trauma, or an idiopathic deficit diagnosed with a stimulation test — replacement therapy with recombinant GH (somatropin) has been standard of care for decades, with indications and dosages defined in guidelines from endocrinological societies. It improves body composition, bone density, lipid profile, quality of life. The Endocrine Society guidelines (Molitch ME et al., J Clin Endocrinol Metab, 2011) and the more recent AACE/ACE update (Yuen KCJ et al., Endocr Pract, 2019) define who must be treated, how, for how long, with what monitoring. It is medicine with a precise purpose: not “stimulating youth”, but correcting a measurable deficit.
HIV-associated lipodystrophy. Tesamorelin has been FDA-approved since 2010 for exactly this indication: it reduces visceral fat in HIV+ patients with lipodystrophy, with efficacy and safety data from randomised trials on more than a thousand participants (Falutz J et al., N Engl J Med, 2007; Stanley TL et al., JAMA, 2014; long-term safety profile in Falutz J et al., AIDS, 2008). It is not an anti-ageing drug, it is a drug for a specific condition with a specific endpoint. The difference seems subtle, it is fundamental: the trial was designed to answer a defined clinical question, not to sell a longevity protocol.
Paediatric GH deficiency and specific syndromes. Recombinant GH and — in selected contexts — Sermorelin are used in paediatric GH deficiency, Turner syndrome, Prader-Willi syndrome, SHOX deficiency, chronic renal insufficiency with growth retardation. These are indications with decades of follow-up, published safety data, consolidated paediatric guidelines.
The boundary with off-label anti-ageing use. In the United States, the distribution or prescription of GH for anti-ageing purposes has been explicitly illegal since 1988 (21 U.S. Code §333(e)) — a norm unique in American pharmacology, conceived precisely to curb a market that was already then pushing cosmetic use. The systematic review by Liu and colleagues (Annals of Internal Medicine, 2007) on thirty-one studies in healthy elderly people showed marginal benefits on body composition, no significant effect on strength or functional capacity, and frequent side effects (oedema, carpal tunnel syndrome, arthralgias, gynaecomastia, glucose intolerance). Daniel Rudman — author in 1990 of the New England Journal of Medicine paper that, misinterpreted, launched the myth of GH as the fountain of youth — publicly distanced himself from anti-ageing use before he died. Those who cite that paper decades later as proof of efficacy rarely also cite the author’s change of heart, nor the counterbalancing literature that followed (Perls TT, Reisman NR, Olshansky SJ, JAMA, 2005).
On CJC-1295 and Ipamorelin — the two most widespread secretagogues in the grey market — the human literature consists of single Phase I/II studies, often sponsored by the companies that wanted to develop them as drugs and that then did not pursue clinical development to approval (Teichman SL et al., J Clin Endocrinol Metab, 2006 for CJC-1295; Raun K et al., Eur J Endocrinol, 1998 for Ipamorelin). Those data exist, they are real, but they do not cover what would be needed to use them as chronic therapy outside a trial.
The point is simple: GH secretagogues have a clinical space, monitored, defined. It is a small island in the middle of an ocean of claims. The island deserves respect. The ocean deserves scepticism.
12. Longevity clinics and regulatory arbitrage¶
If peptides were produced only by Chinese laboratories and bought on obscure websites, the phenomenon would be marginal. It is not. Around peptides a category of clinics has grown in recent years — often presented as longevity clinics, regenerative medicine centers, preventive wellness institutes — which offer them in premium packages, with real medical infrastructure, glossy marketing, and a narrative built around the idea that optimising one’s own biology is not only possible but a duty, at least for those who can afford it.
Dubai is one of the most visible hubs of this economy. Not by chance. The Emirates have explicitly positioned longevity as a strategic sector — public incubators, tax breaks for specialised clinics, partnerships with international brands — within a regulatory framework that allows medical practices difficult or impossible in Europe and the United States. Compounding pharmacies can prepare peptides that the FDA has removed from the list of substances usable in compounding. Doctors can prescribe off-label with less stringent constraints. All this in a private, self-pay context, without the filters of public health insurance, with an international high-end clientele that flies in for a weekend of injections, NAD+ infusions, hyperbaric oxygen therapy and biometric check-ups.
Dubai is not the only one. Monaco, Switzerland with its alpine clinics, the Caribbean for stem cells, Mexico for experimental therapies, Singapore for Asian longevity. It is a global circuit that exploits differences between jurisdictions the way other industries exploit tax differentials: regulatory arbitrage. If a treatment is banned or tightly restricted in one jurisdiction, it is offered in another. The client travels.
Two things must be distinguished, for honesty’s sake.
The first is that some of these clinics also do serious medicine. In-depth screening, preventive diagnostics, personalised endocrinology, monitored hormone replacement therapy. Coming away with an early diagnosis of thyroiditis, with a recalibration of your vitamin D, with legitimate testosterone replacement therapy for real hypogonadism, is plausible. Those who work there often know what they are doing.
The second is that the same clinics, in the same package, tend to include treatments with much weaker evidence — unapproved peptides, vitamin IVs, uncharacterised stem cells, plasmapheresis with rejuvenation claims — presented as components of the same “integrative” approach. The net effect is that the aura of serious medicine in the first half of the package covers the methodological uncertainty of the second. The buyer pays for everything and receives everything. Rarely does anyone separate, in the conversation with the client, what has efficacy data and what does not.
The business model aggravates the problem. The client is not a patient in the classical sense, they are a health optimiser. They do not present with a disease to be cured but with a desire to optimise parameters. The clinic responds with annual packages, memberships, seasonal protocols. The incentive is not to discharge the client when they are well, but to keep them on a continuous pathway where each visit generates new recommendations. It is not necessarily malice; it is how the economic model is built.
The typical client, in turn, is not naive. Often they are informed, they read the literature — whatever comes their way — they know the names of the peptides, they want to participate actively in decisions about their own biology. But informed is not the same thing as equipped to evaluate the primary literature, and the sense of control over one’s own body is one of the goods these clinics sell most effectively. The price of that sense of control, sometimes, is accepting extrapolations that the seller knows they are making and the buyer prefers not to dig into.
It is not a marginal phenomenon. It is a growing industry, with significant capital, with a cultural narrative that is gaining ground in Europe too. Italian and Swiss clinics that are starting to offer “longevity programmes” follow the model, often with fewer grey peptides but with the same conceptual apparatus. It is worth recognising it for what it is: not preventive medicine, not quackery, but a third thing that sits halfway between the two and uses the vocabulary of the first to sell packages that include the second.
Closing: the long time of biology¶
The story of peptides is, in miniature, the same story as longevity.
There is real science behind it: decades of serious research on signalling systems, peptide pharmacology, molecular biology. There is a real gap between the science and consumption: the transition from preclinical to human clinical is the longest, most expensive, least photogenic work in the pharmaceutical craft, and it is exactly the step the grey market skips. And there is an illusion of control: having on hand a molecule with a technical name, a syringe, a protocol gives you the sense of governing your own biology. The sense is not the reality. The reality is one cell a day, for years, receiving a growth signal it might use to heal, to regenerate, or for something else that no one has yet measured.
The scientific method is slow for a reason. Because biology is slow. The windows in which harms emerge, when they exist, are years or decades. Short clinical trials do not see them. Individual testimonies do not see them. Today’s “I feel better” is not information about “what will be happening twenty years from now”. The difference between a drug and a bet is who gathered the data for that horizon.
There is an image, in Mary Shelley’s Frankenstein, that returns when thinking about peptides. It is not the monster. It is Victor stitching together pieces of life taken from other bodies and animating them without fully understanding what he is generating. Enthusiasm for the mechanism — it works, it moves, it breathes — precedes the question about what that creature will do over the years, the seasons, the relationships. Prometheus is powerful and naive at the same time. It is a combination that, in the peptide catalogue, is met more often than its dangerousness deserves.
Biology has time. The companies selling peptides do not. It is a discrepancy worth keeping in mind when reading the next claim, however well presented.
In the next article we’ll reason about what “supplementation” really means — when it makes sense and when it is anxiety in capsules.